Acta Paedagogica Vilnensia ISSN 1392-5016 eISSN 1648-665X
2023, vol. 51, pp. 29–46 DOI: https://doi.org/10.15388/ActPaed.2023.51.2
Distance Learning For Military Doctors in Crisis Situations: The DILEMMA Cross-Sectional Study Results
Nataliia Sydorova
Department of Military General Practice and Family Medicine,
Ukrainian Military Medical Academy, Ukraine
synn.kiev@gmail.com
ORCID 0000-0003-3451-3317
Valerii Savytskyi
Ukrainian Military Medical Academy, Kyiv, Ukraine
savvalleon@ukr.net
ORCID 0000-0001-8027-0163
Taras Kuts
Department of Military General Practice and Family Medicine,
Ukrainian Military Medical Academy, Kyiv, Ukraine
taraskuts@gmail.com
ORCID 0000-0001-7619-3679
Abstract. Background: Distance learning for medical personnel, although convenient in times of crisis (pandemics, military operations), can be a problem in terms of the limited practical component of such training. The goal of presented Survey on DIstance LEarning for students of the Ukrainian Military Medical Academy (DILEMMA) was to optimize the educational process for doctors studying at the Ukrainian Military Medical Academy (UMMA) based on the results of students’ survey dedicated to implemented forms of online teaching. Methods: The data presented reflect the results of 147 trainees’ survey dedicated to their satisfaction and ways to improve distance learning component of training/retraining at UMMA during such crisis situations as pandemics and hostilities. Primary and secondary endpoints were analyzed for groups of interns (DILEMMA-1, n=78) and physicians with practical experience participating in postgraduate activities at UMMA (DILEMMA-2, n=69). Results. The overall evaluations of distance learning as measured by a 10-point scale (primary endpoint) were 5.9±3.3 for DILEMMA-1 and 6.5±3.3 for DILEMMA-2 (p=0.27), which indicates a moderate overall evaluation. The proportion of satisfied and very satisfied students was smaller in the DILEMMA-1 group compared to DILEMMA-2 but remained quite high (76.9% vs. 92.8%, respectively, p<0.05). Respondents of the DILEMMA-1 and DILEMMA-2 arms gave different answers to the questions related to their preferred forms of online education, mode, and schedule. In particular, representatives of the DILEMMA-2 arm mostly prefer to have their online classes after 3:00 p.m. (67.5%) with duration for about 2 hours (56.5%), while most participants in DILEMMA-1 arm (73.1%) choose time interval from 9:00 a.m. to 11:00 a.m. and 62.8% consider the optimal duration to be 3–4 hours of online classes per day. According to results of survey, optimization of distance learning component was made at UMMA. Conclusions. Differences in the perception of distance learning between interns and doctors with practical experience necessitate a differentiated approach to the implementation of distance learning for these groups of students. In addition, the special categories of respondents among students were identified by us, which lead to the destructuring of the response matrix and the nonparametric nature of some data, dictate the need to censor extremely negative (“denialists”) and extremely positive (“pleasers”) respondents when assessing the quality of teaching by anonymous survey of students, and therefore the size of the initial sample depending on contingent should be increased by 16–25%.
Key words: distance education, postgraduate education, military medicine, survey, medical education
Nuotolinis karo gydytojų mokymasis krizinėse situacijose: DILEMMA kryžminio tyrimo rezultatai
Santrauka. Kontekstas: nuotolinis medicinos personalo mokymas yra patogus krizių (pandemijų, karinių operacijų) metu, tačiau toks mokymas gali netikti dėl ribotų praktikos galimybių. Pristatomos Ukrainos karo medicinos akademijos studentų apklausos apie nuotolinį mokymąsi (angl. Survey on DIstance LEarning for students of the Ukrainian Military Medical Academy (DILEMMA) tikslas – optimizuoti Ukrainos karo medicinos akademijoje (UKMA) studijuojančių gydytojų mokymo procesą, remiantis studentų apklausa apie mokymo internetu formas. Metodai: tyrimo duomenys surinkti iš 147 studentų apklausos apie jų pasitenkinimą ir nuotolinio mokymo tobulinimo būdus UKMA tokiose krizinėse situacijose kaip pandemijos ir karo veiksmai. Pirminiai ir antriniai rodikliai buvo analizuojami stažuotojų (DILEMMA-1, n = 78) ir gydytojų, turinčių praktinės patirties bei dalyvaujančių podiplominėse studijose UKMA (DILEMMA-2, n = 69), grupėse. Rezultatai: bendras nuotolinio mokymosi vertinimas, matuojamas 10 balų skale (pirminis rodiklis), buvo 5,9±3,3 DILEMMA-1 grupės ir 6,5±3,3 DILEMMA-2 grupės (p = 0,27), tai rodo vidutinį vertinimą. Patenkintų ir labai patenkintų studentų dalis buvo mažesnė DILEMMA-1 grupėje, palyginti su DILEMMA-2, tačiau vis tiek ji buvo gana didelė (atitinkamai 76,9 % ir 92,8 %, p < 0,05). DILEMMA-1 ir DILEMMA-2 grupių respondentai skirtingai atsakė į klausimus, susijusius su jų pageidaujamomis mokymosi internetu formomis, metodais ir tvarkaraščiu. Pavyzdžiui, DILEMMA-2 grupės dalyviai dažniausiai pageidavo, kad nuotoliniai užsiėmimai vyktų po 15.00 val. (67,5 %) ir truktų apie 2 valandas (56,5 %), o dauguma DILEMMA-1 grupės dalyvių (73,1 %) rinkosi laiką nuo 9.00 iki 11.00 val. ir 62,8 % manė, kad optimali nuotolinių užsiėmimų trukmė yra 3–4 valandos per dieną. Remiantis apklausos rezultatais, UKMA pavyko optimizuoti nuotolinį mokymąsi. Išvados: skirtingas praktikantų ir praktinės patirties turinčių gydytojų požiūris į nuotolinį mokymąsi lemia būtinybę taikyti diferencijuotą požiūrį į nuotolinio mokymosi taikymą šioms studentų grupėms. Be to, tyrime buvo išskirtos tam tikros studentų grupės, kurių atsakymai išryškino būtinybę pakoreguoti galimus atsakymų variantus ir lėmė kai kurių duomenų neparametriškumą bei parodė, kad, vertinant mokymo kokybę anoniminės studentų apklausos būdu, svarbu cenzūruoti itin neigiamus („neigikus“) ir itin teigiamus („pataikūnus“) respondentus, todėl pradinės imties dydį priklausomai nuo sudėties reikėtų padidinti 16–25 %.
Pagrindiniai žodžiai: nuotolinis mokymas, podiplominės studijos, karinė medicina, apklausa, medicinos studijos.
Received: 24/07/2023. Accepted: 20/10/2023
Copyright © Nataliia Sydorova, Valerii Savytskyi, Taras Kuts, 2023. Published by Vilnius University Press. This is an Open Access article distributed under the terms of the Creative Commons Attribution Licence (CC BY), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction
The emergence of crisis situations in countries dictates a change in the process of training doctors both in terms of the subject and forms of education (Kozak et al., 2021; Jain et al., 2022; Sydorova et al., 2022; Remez, 2023). The impact of crisis situations is most noticeable in medical education. The emergence of new diseases dictates the need to change the training program with the introduction of new information; pandemics limit the possibility of practical training and contribute to an increase in the online/distance component of the educational process. In the last few years, the Ukrainian medical education system has faced two challenges: the COVID-19 pandemic and the full-scale invasion of the Russian Federation into the territory of Ukraine. At the same time, the need for training doctors, including military doctors, increased significantly.
In Ukraine, the training and retraining of military doctors is carried out by the Ukrainian Military Medical Academy (UMMA). This institution has been introducing elements of distance learning for several years; a Scientific (educational) Portal has been created as a platform for all online activities of teachers and students (Kozak et al., 2021; Kozak et al., 2023). The procedure and scope of the distance learning component are controlled and studied by the heads of the relevant faculties (Kozak et al., 2021; Kozak et al., 2023). However, there has not been a large-scale assessment of the opinions of the military medical students about the satisfaction of the online component of training with clarification of the needs of trainees of the Faculty of Training of Military Doctors (interns) and the Faculty of Retraining and Advanced Training (continuing postgraduate education). Such a survey at the Academy level, rather than individual departments, will make it possible to more accurately determine convenient forms of online learning and organically fit them into the overall process of training and retraining of doctors, even in crisis situations (Savytskyi et al., 2022).
Literature review
Before the COVID-19 pandemic, learning process in Ukraine and other countries was predominantly unimpaired and the online component was not widely represented. Crisis situations, in particular the COVID-19 pandemic, have led to dramatic changes in teaching in schools, colleges, and higher education institutions (Kozak et al., 2021; Sherman et al., 2022; Mirosavljević et al., 2023). Since the announcement of the first lockdown due to the COVID-19 pandemic in Ukraine, distance education has been experiencing incredibly intensive development in our country (Lucenko et al., 2023). Both synchronous and asynchronous forms of distance learning actively developed at this time, giving educational institutions the opportunity to develop and implement convenient online learning platforms with even virtual classrooms into the educational process (Sherman et al., 2022).
Distance education in medicine has both advantages and disadvantages, the most important of the latter is the lack of practical activities under the supervision of a teacher directly in the clinic (Vasianovych et al., 2023). However, this drawback can be partially eliminated by using a combined form of teaching with the possibility of access to the patient during practical classes or using telemedicine (Poberezhets et al., 2022). In addition, due to the increasing need for distance learning, new forms of teaching are currently being developed and tested that allow for the assimilation of practical skills in an online format: analysis of a clinical case, master classes, interactive clinical tasks with multiple options for the development of a clinical scenario, simulations, role-playing games, etc. (Kozak et al., 2021).
The COVID-19 pandemic has taught educators not only to respond quickly to the need of medical students to receive new information about a previously unknown disease to ensure the best clinical practice, but also led to the widespread introduction of online services – telemedicine and distance learning (Holubnycha et al., 2022; Poberezhets et al., 2022). Since 2020, training at UMMA due to the COVID-19 pandemic has taken place in a mixed form: for interns – situationally, based on the need for self-isolation of groups or individual students/teachers, and for doctors participated in advanced training courses – 50% or even 100% online learning during lockdown (Kozak et al., 2021; Poltorak et al., 2021).
The large-scale Russian invasion of Ukraine has only reinforced these trends (Poberezhets et al., 2022; Sherman et al., 2022; Budko et al., 2023; Remez, 2023; Vasianovych et al., 2023). It should be noted that the proportion of doctors who were trained distantly at the Faculty of Retraining and Advanced Training at UMMA steadily increased from 11% in 2019 (before the pandemic) to 22% in 2020 (first year of COVID-19 pandemic), 42% in 2021 (continuation of the pandemic) and reached a maximum in 2022 – 64% (full-scale Russian invasion of Ukrainian territory) (Kozak et al., 2021).
During the full-scale Russian invasion of Ukraine, especially in its first months, the trend towards online classes dramatically increased, especially for doctors attending postgraduate courses (Khaniukov et al., 2022; Srichawla et al., 2022; Remez, 2023). It should also be noted that higher medical educational institutions, due to the experience gained during the COVID-19 pandemic, were able to quickly organize the process of online training in combat conditions, even for universities in cities located in close proximity to active hostilities (Khaniukov et al., 2022).
The asynchronous form of online learning activities has acquired particular importance in conditions of intermittent access to online classes due to problems with the Internet connection, power blackouts, interruptions of classes due to airraid warnings and bombings (Khaniukov et al., 2022; Sherman et al., 2022). The asynchronous form of online learning as a priority in war conditions was also emphasized in the publication by Taha et al. (2023), who assessed education during war in Sudan. This has led to the intensive development and introduction into the pedagogical process of various online platforms with deposited information for students and access to academic support, which can be required at any time (Galynskaya & Bilous, 2022).
On such a scale, distance learning was not previously used in the country, and discussions about the quality of medical education in distance learning remain open. While the problems of distance undergraduate education have found some reflection in the research publications (Galynska & Bilous, 2022; Holubnycha et al., 2022; Poberezhets et al., 2022; Sherman et al., 2022; Remez, 2023), the issues of postgraduate distance education, especially when it comes to military doctors, whose training requires the development of practical skills and differs from civilian educational process especially in such crisis situations as pandemic or war, have not been studied enough (Kozak et al., 2021; Savytskyi et al., 2022).
Methods
Considering the need to control the quality and satisfaction of trainees with distance learning, it was planned to conduct a cross-sectional study Survey on DIstance LEarning for students of the Ukrainian Military Medical Academy (DILEMMA) with the aim to optimize the educational process for doctors studying at UMMA based on the results of students’ survey dedicated to implemented forms of online teaching (Savytskyi et al., 2022).
The DILEMMA study is a cross-sectional single-center study based on a standardized sample survey in groups of students of the Faculty of Training of Military Doctors (interns) of UMMA (DILEMMA-1 arm, n=78) and students of the Faculty of Retraining and Advanced Training of UMMA (DILEMMA-2 arm, n=69).
The survey was conducted in the period from April 23 to December 26, 2022, but the respondents evaluated their own experience during the entire period of study, that is, from the introduction of distance elements of teaching at UMMA in 2020 due to the COVID-19 pandemic, as well as the experience gained after the start of full-scale hostilities in Ukraine.
The subject of the study was the responses of trainees to the questions posed in the questionnaire about the online component of training at UMMA presented as primary and secondary endpoints expressed in qualitative (degree of satisfaction) and quantitative (10-point scores) characteristics.
Such general information as age and gender of respondents as well as proportion of distance learning were analyzed (Table 1).
The primary endpoint was the general assessment of distance learning by UMMA students (their satisfaction with the distance part of learning expressed as assessment by 10-point score and graduated degree of satisfaction). Additionally, we conducted a subanalysis of components related to the distance learning satisfaction: learning platform organization, impact on practical activities, most interesting for trainees online activities (Table 2).
Secondary endpoints included detailing respondents’ impressions of individual components of the distance learning and interactive activities, namely, advantages and disadvantages of distance learning at UMMA, perspectives of online activities in training/retraining outside of crisis situations such as pandemics and military operations, and most convenient schedule for online activities during training/retraining at UMMA (Tables 3 and 4).
For some questions, respondents were asked to provide answers with a rating from 0 to 10 points and such answers were categorized as follows:
• 0–3 points were considered as minimal impact/negative answer to the question;
• 4–6 points were considered as a neutral answer;
• A score of 7–10 was considered a strong impact/positive response.
The average value of the indicator for each item of the questionnaire and the frequency of scores of categorized blocks for each question were calculated.
The survey was conducted mainly among the students of the Department of Military General Practice and Family Medicine, as well as other clinical departments of UMMA.
The research was conducted in accordance with the requirements of ethics and protection of personal data, the survey was anonymous and voluntary. A link to the Google questionnaire, developed separately for the DILEMMA-1 and DILEMMA-2 groups, was sent to the students from the database of the UMMA Scientific Portal in accordance with the agreement on the use of e-mail data that the students signed when registering on the Portal. The questionnaire did not require filling in any personal data that would allow identification of a person.
Statistical analysis
UMMA students who underwent training during an index period of time were considered as general populations, for which the volumes of sample populations were calculated based on the need to provide the necessary statistical power (1-β) of 90% and the significance level α of 0.05: the minimum calculated number of reviewers was 73 people for the DILEMMA-1 arm, for the DILEMMA-2 arm 51 people.
At the end of the data collection, 78 completed questionnaires were received in the DILEMMA-1 arm, and 69 completed questionnaires in the DILEMMA-2 arm.
When assessing the primary endpoint (overall assessment of distance learning), data were presented as the mean ± standard deviation (M±SD). The distribution of quantitative data in the groups in the vast majority was normal (indicators of kurtosis and asymmetry <2), which made it possible to use, as more accurate, methods of parametric statistics (in this case - a two-sample t-test with different variances). We censored variation series in case of data with a non-normal distribution.
We determined the structure of categorized answers to each question in %, if possible, using the quantification procedure (giving qualitative signs quantitative certainty) for the secondary endpoints. The method of alternative variation was used to compare frequency indicators. Differences at p<0.05 were considered significant.
Microsoft Excel 2010 and the standard statistical package STATISTICA 6.0 were used for calculations.
Results
In the process of analyzing the DILEMMA survey data, we established the presence of additional small peaks at the beginning and the end of the “0–10 points” scale in several variation series of results. The appearance of these peaks led to the nonparametric nature for some parameters, and was found in both surveyed groups. In this regard, we conducted a more thorough examination of the data detailing the results of the survey of specific respondents whose answers formed these additional peaks. This analysis demonstrated the peculiarities of the responses to the questions, which allowed us to identify three groups of DILEMMA-1 respondents:
• Objective respondents had a differentiated approach to questions and answers to them (the majority of respondents, 58 people, 74.4% of cases);
• “Denialists”: when answering most questions, they chose the most negative or negative option (6 people, 7.7%);
• “Pleasers”: when answering most questions, they chose the most positive or positive option (14 people, 17.9% of respondents).
Such data indicate that only about 75% of respondents of the DILEMMA-1 arm really answered responsibly to the survey and evaluated the results of training, giving different directions (positive–negative) and severity (when applying gradations) of answers. The other 25% of respondents gave answers depending on personal motivation (either “everything is bad” – the group of “denialists” or “everything is great” – the group of “pleasers”). It was the survey results of these two groups of respondents that created additional peaks at the beginning and end of the scale and, to some extent, distorted the results. Probably, when planning further research with surveying interns whose epidemiological characteristics are comparable to DILEMMA-1 indicators, it is advisable to increase the size of the sample volume calculated according to standard methods by 25.6% (7.7+17.9%) for possibility, if needed, of further correction of variation series with exclusion (censoring) data from these two anomalous peaks as not carrying objective information.
The analysis of the DILEMMA-2 arm also revealed the presence of “denialists” (5 people, 7.2% of respondents) and “pleasers” (6 people, 8.7% of respondents) but in a smaller number than among the DILEMMA-1 contingent. In general, the number of respondents in the DILEMMA-2 group who gave mostly negative or mostly positive answers to most of the survey questions was 11 people (15.9% of the respondents), therefore, in our opinion, a correction of the calculated sample size should be introduced when surveying a similar contingent with increasing it by 16% and the following censoring in order to more objectively reflect the real picture of the survey and preserve the parametric nature of all presented data.
According to the research design and the calculated volume of the sample population, 78 trainees of the Faculty of Training of Military Doctors of UMMA (interns, DILEMMA-1) were interviewed, most of whom were aged 20–29 (96.2% in total) and men (53 people, 67.9% of respondents), which corresponds to the gender characteristics of the composition of UMMA military interns (see Table 1).
Respondents of the DILEMMA-2 arm were expected to be over 30 years old (95.7%), including 20 people (29.0%) over 50 years old, and the vast majority of respondents were women (47 respondents, 68.1%). The specified feature is also related to the contingent of doctors who study at such courses, which involve not only military servicemen, but also civilian family medicine doctors, physicians from outpatient medical institutions of the Ministry of Defense of Ukraine.
According to the survey of the DILEMMA-1 arm, the proportion of distance learning averaged 57.0±28.9% of the curriculum (see Table 1), i.e., in general, the training received by the respondents can be considered as training under a mixed system, in the structure of which distance learning slightly dominated. It should be noted separately the significant variability of this indicator in the answers of the DILEMMA-1 arm, which was associated with the conditions of the COVID-19 pandemic (introduction of lockdowns with the need to conduct classes only online, transfer of groups with sick people to self-isolation mode) and hostilities on the territory of Ukraine, which, by their dynamics, influenced the possibilities of conducting off-line classes. The respondents’ answers reflect the real picture of the conditions in which training took place, when all cycles at the departments were prepared for teaching in two formats: face-to-face and distance learning. Both forms were provided with access to educational materials on the Scientific Portal of the UMMA, and the form of teaching was chosen depending on the current situation, but if possible, preference was always given to the face-to-face form.
The proportion of distance learning in the DILEMMA-2 group averaged 83.0±25.0% of the curriculum, which is significantly higher than the DILEMMA-1 indicator (р=3.4Е-08). In more than half of the cases, students of this arm underwent 100% distance learning (38 people, 55.1%). This situation corresponds to the regulatory organizational situation, when according to the orders of the relevant ministries, both in the conditions of the pandemic and during the martial law, postgraduate education had to be carried out online.
Table 1. General characteristics for DILEMMA-1 and DILEMMA-2 arms
|
Indicator
|
DILEMMA-1
(n=78)
|
DILEMMA-2
(n=69)
|
p-value
|
|
1. Age range of participants (n, %)*
|
|
20–24 years old
|
35 (44.9%)
|
0
|
|
|
25–29 years old
|
40 (51.3%)
|
3 (4.3%)
|
|
|
≥30 years old
|
3 (3.8%)
|
66 (95.7%)
30–39: 20 (29.0%)
40–49: 26 (37.7%)
≥50: 20 (29.0%)
|
|
|
*We didn’t conduct statistical analysis for these answers because age is associated with group of trainees (interns or experienced doctors)
|
|
2. Male gender
|
53 (67.9%)
|
22 (31.9%)
|
˂0.001
|
|
3. Proportion of distance learning, %
|
|
100%
|
11 (14.1%)
|
38 (55.1%)
|
˂0.001
|
|
90%
|
7 (9.0%)
|
4 (5.8%)
|
>0.05
|
|
80%
|
8 (10.3%)
|
10 (14.5%)
|
>0.05
|
|
70%
|
8 (10.3%)
|
4 (5.8%)
|
>0.05
|
|
60%
|
3 (3.8%)
|
1 (1.4%)
|
>0.05
|
|
50%
|
10 (12.8%)
|
6 (8.7%)
|
>0.05
|
|
40%
|
6 (7.7%)
|
2 (2.9%)
|
>0.05
|
|
30%
|
15 (19.2%)
|
0
|
˂0.001
|
|
20%
|
5 (6.4%)
|
1 (1.4%)
|
>0.05
|
|
10%
|
5 (6.4%)
|
3 (4.3%)
|
>0.05
|
|
Mean proportion for the group, %
|
57.0±28.9
|
83.0±25.0
|
3.4Е-08
|
The overall assessment of distance learning on a 10-point scale (primary endpoint) was 5.9±3.3 points for DILEMMA-1, although the majority of respondents (60 people, 76.9% of respondents) noted satisfaction with the training course, including 18 people (23.1% of respondents) who were “very satisfied” (see Table 2).
The indicator of the primary endpoint in the DILEMMA-2 group was slightly higher, but without a significant difference, amounting to 6.5±3.3 points, although in this group the respondents were reliably more often “satisfied” with the distance component of their education (69.6% of respondents comparing with 53.8% DILEMMA-1 arm, p<0.05) and less frequently rated it as “nothing special” (7.2 vs. 21.8%, respectively, p<0.01).
Responders of DILEMMA-2 were significantly more satisfied with the organization of the educational platform: the average score was 9.0±1.5 vs. 7.4±2.5 points in DILEMMA-1 (р=4.01Е-06).
Table 2. Primary endpoint and its components for DILEMMA-1 and DILEMMA-2 arms
|
Indicator
|
DILEMMA-1
(n=78)
|
DILEMMA-2
(n=69)
|
p-value
|
|
1. Assessment of students’ satisfaction with the distance part of learning
|
|
Mean, points
|
5.9±3.3
|
6.5±3.3
|
0.2663
|
|
2. How satisfied are you with distance learning?
|
|
Very satisfied
|
18 (23.1%)
|
16 (23.2%)
|
>0.05
|
|
Satisfied
|
42 (53.8%)
|
48 (69.6%)
|
˂0.05
|
|
Nothing special
|
17 (21.8%)
|
5 (7.2%)
|
˂0.01
|
|
Dissatisfied
|
1 (1.3%)
|
0
|
>0.05
|
|
3. How satisfied are you with learning platform organization?
|
|
Less satisfied
|
8 (10.3%)
|
1 (1.4%)
|
˂0.05
|
|
Nothing special
|
15 (19.2%)
|
6 (8.7%)
|
>0.05
|
|
More satisfied
|
55 (70.5)
|
62 (89.9%)
|
˂0.001
|
|
Mean, points
|
7.4±2.5
|
9.0±1.5
|
4.01E-06
|
|
4. To what extent distance learning has positively affected your practical activities?
|
|
Helped a lot
|
10 (12.8%)
|
18 (26.1%)
|
˂0.05
|
|
Helped
|
51 (65.4%)
|
48 (69.6%)
|
>0.05
|
|
Didn’t really help
|
13 (16.7%)
|
3 (4.3%)
|
˂0.05
|
|
Did not help at al
|
4 (5.1%)
|
0
|
>0.05
|
|
5. What forms of interactive activities during distance learning did you like?
(multiple answers possible)
|
|
Testing
|
37 (47.4%)
|
37 (53.6%)
|
>0.05
|
|
Clinical tasks
|
51 (65.4%)
|
28 (40.6%)
|
˂0.001
|
|
Video lectures
|
61 (78.2%)
|
52 (75.4%)
|
>0.05
|
|
Students’ reports
|
15 (19.2%)
|
11 (15.9%)
|
>0.05
|
|
Additional website data
|
42 (53.8%)
|
33 (47.8%)
|
>0.05
|
|
Analysis of electrocardiogram, etc.
|
54 (69.2%)
|
30 (43.5%)
|
˂0.001
|
|
Analysis of clinical cases (master classes)
|
60 (76.9%)
|
39 (56.5%)
|
˂0.001
|
|
Role tasks „patient–doctor“
|
33 (42.3%)
|
12 (17.4%)
|
˂0.001
|
A significant positive impact on further practical activity was significantly more often noted by respondents of the DILEMMA-2 arm compared to interns (26.1 vs. 12.8%, p<0.05), while representatives of the DILEMMA-1 arm significantly more often noted the absence of a real distance learning impact for their practice (16.7 vs. 4.3%, respectively, p<0.05).
We determined the main differences in the preferences regarding certain forms of interactive activities during online classes (Figure). However, it should be noted that the respondents of both arms noted video lectures as the most interesting forms of distance learning (78.2% of DILEMMA-1 and 75.4% of DILEMMA-2). It is interesting that respondents considered short messages prepared by students to be the least informative (19.2% of DILEMMA-1 and 15.9% of DILEMMA-2). In our opinion, the listeners’ low interest in short messages is related to the direct need for respondents to prepare such messages themselves.
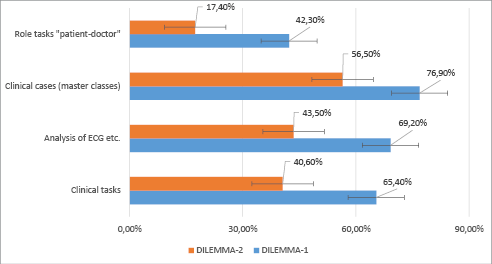
Figure. Respondents’ interest in interactive activities, regarding which the opinion of respondents of both groups significantly differed. The percentage of respondents who positively assessed an index online activity is presented. P-value in all cases <0.001. ECG – electrocardiogram.
Table 3 presents the results of a survey of respondents regarding their assessment of components of the distance learning course (secondary endpoints).
Table 3. Evaluation of the components of distance learning (secondary endpoints) based on the results of a survey of participants from DILEMMA-1 and DILEMMA-2 arms
|
Indicators
|
DILEMMA-1
(n=78)
|
DILEMMA-2
(n=69)
|
p-value
|
|
Indicators
|
DILEMMA-1
(n=78)
|
DILEMMA-2
(n=69)
|
p-value
|
|
1. No need to come to the location
|
|
Less satisfied
|
2 (2.6%)
|
3 (4.3%)
|
>0.05
|
|
Nothing special
|
5 (6.4%)
|
4 (5.8%)
|
>0.05
|
|
More satisfied
|
71 (91.0%)
|
62 (89,9%)
|
>0.05
|
|
Mean, points
|
9.2±1.9
|
8.9±2.0
|
0.2923
|
|
2. Access to videos of master classes
|
|
Less satisfied
|
0
|
1 (1.4%)
|
>0.05
|
|
Nothing special
|
5 (6.4%)
|
4 (5.8%)
|
>0.05
|
|
More satisfied
|
73 (93.6%)
|
64 (92.8%)
|
>0.05
|
|
Mean, points
|
9.4±1.3
|
9.3±1.7
|
0.5226
|
|
3. Convenient test control
|
|
Less satisfied
|
2 (2.6%)
|
1 (1.4%)
|
>0.05
|
|
Nothing special
|
12 (15.4%)
|
8 (11.6%)
|
>0.05
|
|
More satisfied
|
64 (82.0%)
|
60 (87.0%)
|
>0.05
|
|
Mean, points
|
8.6±2.0
|
8.6±1.9
|
0.9849
|
|
4. Helpful additional materials on website
|
|
Less satisfied
|
7 (9.0%)
|
0
|
>0.05
|
|
Nothing special
|
13 (16.7%)
|
8 (11.6%)
|
>0.05
|
|
More satisfied
|
58 (74.3%)
|
61 (88.4%)
|
˂0.05
|
|
Mean, points
|
7.8±2.7
|
8.9±1.6
|
0.0040
|
|
5. Consistency of tests with lecture material
|
|
Less satisfied
|
10 (12.8%)
|
2 (2.9%)
|
˂0.05
|
|
Nothing special
|
18 (23.1%)
|
9 (13.0%)
|
>0.05
|
|
More satisfied
|
50 (64.1%)
|
58 (84.1%)
|
˂0.001
|
|
Mean, points
|
7.2±2.7
|
8.4±1.9
|
0.0026
|
|
6. Interactivity level
|
|
Less satisfied
|
3 (3.8%)
|
0
|
>0.05
|
|
Nothing special
|
22 (28.2%)
|
13 (18.8%)
|
>0.05
|
|
More satisfied
|
53 (68.0%)
|
56 (81.2%)
|
>0.05
|
|
Mean, points
|
7.7±2.4
|
8.2±1.7
|
0.1395
|
|
7. Representation of real clinical practice in distance learning
|
|
Less satisfied
|
7 (9.0%)
|
27 (39.1%)
|
˂0.001
|
|
Nothing special
|
16 (20.5%)
|
12 (17.4%)
|
>0.05
|
|
More satisfied
|
55 (70.5%)
|
30 (43.5%)
|
˂0.001
|
|
Mean, points
|
7.6±2.5
|
5.3±3.7
|
0.0024
|
|
8. Presence of clinical case analysis
|
|
Less satisfied
|
18 (23.1%)
|
31 (44.9%)
|
˂0.001
|
|
Nothing special
|
16 (20.5%)
|
14 (20.3%)
|
>0.05
|
|
More satisfied
|
44 (56.4%)
|
24 (34.8%)
|
˂0.001
|
|
Mean, points
|
6.1±3.3
|
4.4±3.5
|
0.0024
|
|
9. Technical convenience: internet connection, etc.
|
|
Less satisfied
|
31 (39.7%)
|
38 (55.1%)
|
>0.05
|
|
Nothing special
|
25 (32.1%)
|
12 (17.4%)
|
˂0.05
|
|
More satisfied
|
22 (28.2%)
|
19 (27.5%)
|
>0.05
|
|
Mean, points
|
4.5±2.9
|
3.9±3.2
|
0.3024
|
|
10. Convenient training arrangement
|
|
Less satisfied
|
1 (1.3%)
|
2 (2.9%)
|
>0.05
|
|
Nothing special
|
25 (32.1%)
|
9 (13.0%)
|
˂0.01
|
|
More satisfied
|
52 (66.7%)
|
58 (84.1%)
|
˂0.01
|
|
Mean, points
|
7.4±2.1
|
8.5±1.9
|
0.0517
|
In the DILEMMA-1 arm, the highest average rating was given to such components as the possibility of watching master classes (mean 9.4±1.3 points, 93.6% of favorable reviews), the absence of the need to travel to the place of study (mean 9.2±1.9 points, 91.0% of favorable reviews), and convenience of test control (mean 8.6±2.0 points, 82.1% of favorable reviews).
Respondents of the DILEMMA-2 arm most liked the possibility of watching master classes (mean 9.3±1.7 points), the absence of the need to travel to study location (mean 8.9±2.0 points), the availability of materials on the Scientific Portal (mean 8.9±1.6 points), and the convenience of test control (mean 8.6±1.9 points).
During the comparative analysis, no statistical differences were found in the answers of the respondents of both groups regarding the need to come to the place of study, access to videos of master classes, the convenience of test control, the level of interactivity during the lesson, and technical convenience. At the same time, respondents of DILEMMA-2 had a significantly more positive attitude to such components as “helpful additional materials on website,” “consistency of tests with lecture material,” “convenient training arrangement” (see Table 3) but they were reliably less satisfied, compared to DILEMMA-1 students, to such components as the “representation of real clinical practice in distance learning,” and “presence of clinical case analysis” (see Table 3). The obtained results indicate the need to review materials for classes with experienced doctors and increase the number of clinical case discussions, in particular, real ones from clinical practice.
Interesting from the point of view of the organization of the learning process at UMMA were the results of the survey, devoted to the perspective of students’ participation in the activities of UMMA postgraduate education (see Table 4). Thus, 83.3% of DILEMMA-1 respondents and 82.6% of DILEMMA-2 respondents have a desire to participate in events with distance forms of learning at UMMA in the future, somewhat less (75.6 and 56.5%, respectively) in events with a mixed form of learning. It should be noted that representatives of DILEMMA-2 significantly more often compared to those of DILEMMA-1 preferred completely online classes (43.5 vs. 24.4%, respectively, p<0.001) and significantly less often chose the mixed format (see Table 4).
Although both groups considered the most convenient duration of the postgraduate study courses to be 2–3 days, students of the DILEMMA-1 arm chose this option significantly more often (76.9%, compared to 49.3% of the respondents of the DILEMMA-2 arm, p<0.001).
The preferences of both groups regarding the duration of the distance component of the classes and the optimal time period for such classes turned out to be different. DILEMMA-1 responders mostly chose classes lasting 3–4 hours (62.8%), less often a 2-hour classes (35.9%), while more than half of DILEMMA-2 respondents chose a 2-hour classes, and almost a third 1-hour classes (p in all cases <0.001). In addition, DILEMMA-1 students considered the optimal time for conducting online classes before lunch, while doctors from the DILEMMA-2 arm by two-thirds of the respondents determined the optimal time to be after 3:00 p.m. (p in all cases <0.001).
The answers of the representatives of both groups to the questions regarding the recommendation of UMMA postgraduate education courses to other doctors under the conditions of free or paid participation, as well as the reasons for choosing the online courses in the future, were mostly expected (see Table 4).
Table 4. Perspectives of distance education of doctors and desirable schedule of online activities during training/retraining according to the results of a survey of DILEMMA-1 and DILEMMA-2 participants
|
Indicators
|
DILEMMA-1
(n=78)
|
DILEMMA-2
(n=69)
|
p-value
|
|
1. Would you like distance education to remain in the usual conditions?
|
|
Yes
|
65 (83.3%)
|
57 (82.6%)
|
>0.05
|
|
No
|
13 (16.7%)
|
12 (17.4%)
|
>0.05
|
|
2. Which format of distance learning do you prefer?
|
|
Fully distance learning
|
19 (24.4%)
|
30 (43.5%)
|
˂0.001
|
|
Mixed format
|
59 (75.6%)
|
39 (56.5%)
|
˂0.01
|
|
3. What is the duration of the distance learning course you are interested in
(you can choose several)
|
|
One day
|
25 (32.1%)
|
16 (23.2%)
|
>0.05
|
|
2–3 days
|
60 (76.9%)
|
34 (49.3%)
|
˂0.001
|
|
One week
|
24 (30.8%)
|
19 (27.5%)
|
>0.05
|
|
Two weeks
|
8 (10.3%)
|
11 (15.9%)
|
>0.05
|
|
4. How many hours would you like to spend daily during distance learning courses
(you can choose several)?
|
|
1 hour
|
3 (3.8%)
|
20 (29.0%)
|
˂0.001
|
|
2 hours
|
28 (35.9%)
|
39 (56.5%)
|
˂0.001
|
|
3–4 hours
|
49 (62.8%)
|
13 (18.8%)
|
˂0.001
|
|
Full day (ca. 8 hours)
|
11 (14.1%)
|
2 (2.9%)
|
˂0.01
|
|
5. What period of the day is more convenient for you to do distance learning
(you can choose several)
|
|
9.00–11.00
|
57 (73.1%)
|
8 (11.6%)
|
˂0.001
|
|
11.00–13.00
|
40 (51.6%)
|
10 (14.5%)
|
˂0.001
|
|
13.00–15.00
|
15 (19.2%)
|
9 (13.0%)
|
>0.05
|
|
After 15.00
|
7 (9.0%)
|
45 (67.5%)
|
˂0.001
|
|
6. What is the main reason for choosing a distance learning course in the future for you?
|
|
Study without the main job interruption
|
38 (48.7%)
|
38 (55.1%)
|
>0.05
|
|
Study without leaving the place of living
|
16 (20.5%)
|
11 (15.9%)
|
>0.05
|
|
Study in short courses
|
12 (15.4%)
|
3 (4.3%)
|
˂0.05
|
|
Useful information presented in a concise manner
|
10 (12.8%)
|
6 (8.7%)
|
>0.05
|
|
More interesting topics
|
0
|
10 (14.5%)
|
˂0.05
|
|
Easier to learn
|
0
|
1 (1.4%)
|
>0.05
|
|
A combination of several reasons
|
2 (2.6%)
|
0
|
>0.05
|
|
7. Would you recommend distance learning courses (free of charge)
of this institution to other doctors?
|
|
Definitely recommend
|
27 (34.6%)
|
33 (47.8%)
|
>0.05
|
|
Rather yes
|
42 (53.8%)
|
29 (42.0%)
|
>0.05
|
|
Don’t know
|
8 (10.3%)
|
5 (7.2%)
|
>0.05
|
|
Rather no
|
1 (1.3%)
|
2 (2.9%)
|
>0.05
|
|
8. Would you recommend distance learning courses (for a fee)
of this institution to other doctors?
|
|
Definitely recommend
|
12 (15.4%)
|
18 (26.1)
|
>0.05
|
|
Rather yes
|
31 (39.7%)
|
34 (49.3%)
|
>0.05
|
|
Don’t know
|
27 (34.6%)
|
15 (21.7%)
|
>0.05
|
|
Rather no
|
8 (10.3%)
|
2 (2.9%)
|
>0.05
|
Discussion
The method of surveying trainees and doctors is effective in determining optimization needs and determining priority directions for improving the training process and is widely used (Kalke et al., 2022; Poberezhets et al., 2022). However, no survey of students regarding distance education in institutions training military doctors has been conducted so far.
To date, there are only a few surveys of students in higher education institutions regarding distance education in crisis situations (Lucenko et al., 2023, Mayer et al., 2023). However, the goals and objectives of such surveys do not correspond to those when assessing education in a military institution. For example, in the study by Lucenko et al. (2023), where they assessed the opinions about distance education during COVID-19 pandemic of 110 students from two pedagogical universities in Ukraine, respondents noted as advantages of distance learning the absence of a dress code and the ability not to turn on the camera (prohibited during online classes at UMMA) and the opportunity to study anywhere in the world at any time, while UMMA trainees could only be in Ukraine and the bulk of the remote training took place online at set hours. Students from pedagogical universities indicated a lack of social contacts and an unstable Internet connection as disadvantages in this study (Lucenko et al., 2023). However, distance learning was limited to episodes of lockdown or self-isolation of the group for up to two weeks maximum at UMMA during the COVID-19 pandemic, and significance for education instability of the Internet connection was observed in a short period October–November 2022 during power blackouts in Ukrainian cities due to bombing by Russia; this problem was subsequently eliminated for military institutions.
Mayer et al. (2023) conducted a survey of 190 students from various medical schools in Ukraine in October–November 2022 with a focus on wartime education. But again, the issues that were studied in it are of little information for optimizing training specifically at UMMA. Thus, the issues of interruption of education (this did not occur at UMMA), the psychological and financial problems of students, in particular those who left the country, as well as issues of international cooperation were examined especially carefully by Mayer et al. (2023). Most of these problems are solved primarily centrally at UMMA, all students remained in Ukraine, and international cooperation in wartime conditions differed significantly from that of civilian universities. In that study, the most popular online learning activities by attendance were workshops (65%), lectures (63%), seminars (39%), Learning-Management-Systems (34%), screencasts/videos (24%) (Mayer et al., 2023).
A feature of our research is the clarification of the most popular online activities not only for students completing medical training (interns) but also for postgraduate students and doctors with experience, which makes it possible to optimize the educational process in the most targeted manner. According to the design, the DILEMMA study included various contingents of UMMA students – interns who are mostly military personnel and undergo training for another 2–3 years depending on specialization after graduating from a civilian institution of higher medical education (DILEMMA-1), and mainly civilian doctors of a therapeutic profile who participated in advanced education events to obtain the required annual number of advanced education points according to the legislation of Ukraine – DILEMMA-2 (Poltorak et al., 2021; Remez, 2023).
Thus, for representatives of DILEMMA-1, the top 5 online activities included video lectures (78.2%), analysis of clinical cases (somewhat similar to workshops, 76.9%), analysis of the electrocardiogram, etc. (65.4%), additional website data (53.8%). Moreover, these activities were noted by more than half of the trainees of the DILEMMA-1 arm, which was not observed in the study by Mayer et al. (2023). Representatives of the DILEMMA-2 arm were somewhat less optimistic, and although the top 5 remained almost unchanged in composition, the preferences of doctors with experience in postgraduate education courses differed from those of DILEMMA-1 arm: video lectures (75.4%), analysis of clinical cases (56.5%), testing (53.6%), additional website data (47.8%), electrocardiogram analysis, etc. (43.5%). These results provide an opportunity for educators of UMMA to reorient their distance teaching to accommodate these individual needs.
In our study, the proportion of distance learning indicated by respondents was slightly different from previous literature data, namely, Kozak et al. (2023) mentioned in their analysis that 64% of trainees of the Faculty of Retraining and Advanced Training of UMMA were studied distantly in 2022, while in our survey the average measure stated by respondents was 83.0±25.0% for this faculty, and slightly less (57.0±28.9%) for interns. Such differences in the percentage of distance learning for the same faculty are explained primarily by different estimates of the indicator: the percentage of students who studied remotely was assessed in the study conducted by Kozak et al. (2023), while in our survey we asked respondents to indicate the average percentage of class time when learning was carried out online. It is obvious that in 2022, before the start of Russian full-scale invasion of the territory of Ukraine, training, with the exception of rare cases of quarantine measures due to the COVID-19 pandemic, was carried out in the usual onsite mode, and, after the start of hostilities, teaching at the Faculty of Retraining and Advanced Training was carried out entirely online. Moreover, the frequency of online classes for interns was also high in the first months of hostilities. Therefore, each participant in the DILEMMA survey reflected their own experience in their answers.
Understanding the needs and requests of students in the field of new teaching methods, in particular digital and/or distance ones, will make it possible to better adjust the teaching process, determine the needs for teacher training, increase their technical skills and create conditions for better student engagement (Girdzijauskienė et al., 2022; Holubnycha et al., 2022; Budko et al., 2023). It is clear that the war in Ukraine will continue for some time and the distance education component, especially in the context of advanced medical education, will remain significant (Jain et al., 2022; Srichawla et al., 2022; Vasianovych et al., 2023).
This was the rationale for significant differences between the groups of respondents who were interviewed. In addition, the attitude of respondents to distance learning and its components also differed in both arms of the respondents, which makes it possible not only to adjust the educational process for each group, but also to optimize the work of the departments as such.
As a result, a number of implementations were introduced at UMMA. Thus, thanks to the research carried out, at the Department of Military General Practice andFamily Medicine and the Academy as a whole, measures were introduced to improve the online component of education: short distance learning courses were introduced for students of the Faculty of Retraining and Advanced Training, in particular, one-day trainings and two-day professional schools with maximum exposure of all materials on the Scientific Portal of UMMA. Emphasis is placed on certain forms of online activities depending on the preferences of the students, the wishes of the students regarding the schedule of online classes are taken into account, a database of additional publications and other useful information is being developed, in particular the electronic library of the institution.
The study had certain limitations. This was a single-center study performed at higher education institution of the Ministry of Defense of Ukraine, so extrapolation of its results to other institutions should be done with caution. Although the sample sizes after the completion of the data collection were larger than the prespecified ones, for the DILEMMA-1 arm the percentage of excess was 6.9%, for DILEMMA-2 it was 35.3%. Thus, after the analysis and determination of respondents whose answers due to our findings of “denialists” and “pleasers” would be better to censor in order to preserve the objective and parametric consistency of the data, the DILEMMA-1 sample did not allow for a full 25% censoring of “denialists” and “pleasers” in this arm. Anyway, such a feature was not yet known to us and was not described in the available literature before the start of the statistical analysis at the end of the collection of questionnaires. This information will be considered in our future surveys.
It should be noted that the groups were not homogeneous in terms of age and gender, but this difference was due to the peculiarities of the internship and postgraduate education. Although the questionnaire contained questions with the explanation that the survey concerns only the distance learning component, it cannot be ruled out that the respondents still evaluated the teaching process as a whole. The last limitation of the study may be that the respondents of the DILEMMA-1 arm participated in different content modules online, which was due to the change in the situation during the pandemic and hostilities. These modules were prepared by different teachers and could differ from each other in the level of basic and additional materials, the manner of online teaching and technical skills of the teacher, his/her ability to respond to technical problems during connection.
Conclusions
1. According to the data of the 2022 survey DILEMMA, the total percentage of distance learning during postgraduate education for intern doctors of the UMMA (DILEMMA-1) was 57.0±28.9%, for doctors with experience (DILEMMA-2) it was 83.0±25.0% (p=3.4E-08), which is related to the peculiarities of the COVID-19 pandemic course and hostilities on the territory of Ukraine.
2. The analysis of the DILEMMA survey results showed that students were not completely satisfied with the results of the distance learning component at UMMA. This is evidenced by the moderate total score of the distance learning assessment: the overall evaluation of distance learning on a 10-point scale (primary endpoint) was 5.9±3.3 for the DILEMMA-1 arm and 6.5±3.3 for DILEMMA-2 (p=0.27). However, the proportion of satisfied and very satisfied students, although it was lower in the DILEMMA-1 compared to DILEMMA-2, remained quite high (76.9 vs. 92.8%, respectively, p<0.001).
3. Respondents of the DILEMMA-1 and DILEMMA-2 arms gave different answers to the questions related to preferences regarding the forms of online education, mode and schedule. In particular, representatives of the DILEMMA-2 arm mostly want to work out after 3:00 p.m. (67.5%) for about 2 hours (56.5%), while 73.1% of DILEMMA-1 respondents prefer to work out from 9:00 a.m. to 11:00 a.m., and they consider the optimal duration to be 3–4 hours of online classes per day (62.8% of respondents).
4. Considering the presence of respondents who tend to give only extremely negative answers to most questions (defined as “denialists”, 7.7% for DILEMMA-1 arm and 7.2% for DILEMMA-2 arm) or only extremely positive answers (defined as “pleasers”, 17.9% for DILEMMA-1 arm and 8.7% for DILEMMA-2 arm), a sample size correction for surveys of a similar contingent should be introduced in the form of adding 25% when surveying interns and 16% when surveying doctors with experience, with subsequent censoring of answers these “extreme respondents.”
Funding. The study was conducted without funding.
Conflict of interest. The authors declare no conflict of interest
References
Budko, H., Ivakhniuk, T., Ivakhniuk, Y., Plakhtiienko, I., & Tsekhmister, Y. (2023). Digital education hubs in medical higher education: Ukraine and the EU perspectives. Amazonia Investiga, 12(63), 233–242. https://doi.org/10.34069/AI/2023.63.03.22.
Galynska, O., & Bilous, S. (2022). Remote learning during the war: challenges for higher education in Ukraine. International Science Journal of Education & Linguistics, 1(5), 1–6. https://doi.org/10.46299/j.isjel.20220105.01.
Girdzijauskienė, R., Norvilienė, A., Šmitienė, G., & Rupšienė L. (2022). Strengthening Student Engagement in Learning Through Use of Digital Tools. Acta Paedagogica Vilnensia, 49, 115–130. Doi: 10.15388/ActPaed.2022.49.8. [In Lithuanian].
Holubnycha, L., Besarab, T., Pavlishcheva, Y., Kadaner, O., & Khodakovska O. (2022). E-Learning at the Tertiary Level in and After Pandemic. Acta Paedagogica Vilnensia, 48, 47–60. Doi: 10.15388/ActPaed.2022.48.3.
Jain, N., Panag, D. S, Srivastava, M., et al. (2022). Fate and future of the medical students in Ukraine: A silently bubbling educational crisis. Med Educ, 56(8), 779–782. Doi:10.1111/medu.14818.
Kaļķe, B., Baranova, S., & Āboltiņa, L. (2022). Self-Assessment of the Professional Competence of Preschool Teaching Student. Acta Paedagogica Vilnensia, 48, 116–128. Doi: 10.15388/ActPaed.2022.48.7.
Khaniukov, О. О., Smolianova, O. V., & Shchukina, O.S. (2022). Distance learning during the war in Ukraine: experience of internal medicine department (organisation and challenges). Art of Medicine, 3(23), 134–138. Doi: 10.21802/artm.2022.3.23.134.
Kozak, N. D., Rudynckyi, O. V., & Kozak, D. O. (2023). Osoblyvosti orhanizatsii navchalnoho protsesu na fakulteti perepidhotovky ta pidvyshchennia kvalifikatsii Ukrainskoi viiskovo-medychnoi akademii v umovakh voiennoho stanu [Features of the educational process organization at the faculty of retraining and advanced training of the Ukrainian Military Medical Academy in the conditions of martial law]. Current Aspects of Military Medicine, 30(1), 38–47. https://doi.org/10.32751/2310-4910-2023-30-1-03. [In Ukrainian].
Kozak, N., Rudynskyi, O., & Kozak, D. (2021) Pilot study applying distance learning during continuous professional development of military doctors in Ukrainian Military Medical Academy. Current Aspects of Military Medicine, 28(1), 10–24. Doi: 10.32751/2310-4910-2021-28-1-01.
Lucenko, G. Lutsenko, O., Tiulpa, T., Sosnenko, O., & Nazarenko, O. (2023). Online - Education and training in higher educational institutions of Ukraine: Challenges and benefits. International Journal of Educational Research Open, 4. 100231. Doi: 10.1016/j.ijedro.2023.100231.
Mayer, A., Yaremko, O., Shchudrova, T., Korotun, O., Dospil, K., & Hege, I. (2023). Medical education in times of war: a mixed-methods needs analysis at Ukrainian medical schools. BMC medical education, 23(1), 804. https://doi.org/10.1186/s12909-023-04768-2.
Mirosavljević, A., Bognar, B. & Sablić, M. (2023) Opportunities and Challenges in the Work of Natural Science Teachers During Online Teaching: Teachers’ Beliefs and Attitudes. Acta Paedagogica Vilnensia, 50, 88–106. Doi:10.15388/ActPaed.2023.50.6.
Poberezhets, V., Demchuk, A., & Mostovoy, Yu. (2022). How Russian-Ukrainian War Changed the Usage of Telemedicine: A Questionnaire-Based Study in Ukraine. Ankara Med J, 22(3), 305–318. Doi:10.5505/amj.2022.08455.
Poltorak, M. F., Orda, M. V., Kozak, N. D., Levitska, L. A., & Bielozorova, O. V. (2021). Svitovi tendentsiy rozvytku dystantsiynoho navchannya: systemoutvoryuyuchi faktory systemy dystantsiynoho navchannya u vyshchykh viysʹkovykh navchalʹnykh zakladakh [World trends in the development of distance learning: system-forming factors of the system of distance learning in higher military schools]. Ukrainian Journal of Military Medicine, 2(1), 19–27. https://doi.org/10.46847/ujmm.2021.1(2)-019. [In Ukrainian].
Remez, D. (2023). Overview of Medical Education in Ukraine. Igaku Kyoiku/ Medical Education (Japan), 53(6), 502–511, https://doi.org/10.11307/mededjapan.53.6_502.
Savytskyi, V. L., Kutz, T. V., & Sydorova, N. M. (2022). Otsinka orhanizatsiyi ta yakosti dystantsiynoho navchannya likariv v kryzovykh sytuatsiyakh: obgruntuvannya ta dyzayn doslidzhennya DILEMMA [Evaluation of the organization and quality of medical distance learning in crisis situations: rationale and design of the DILEMMA survey]. Current Aspects of Military Medicine, 29, 29–38. https://doi.org/10.32751/2310-4910-2022-29-3. [In Ukrainian].
Sherman, M., Puhovskiy, E., Kambalova, Y., & Kdyrova, I. (2022). The Future of Distance Education in War or the Education of the Future (The Ukrainian Case Study). Futurity Education, 2(3), 14–23. https://doi.org/10.57125/FED/2022.10.11.30.
Srichawla, B.S., Khazeei Tabari, M. A., Gaman, M. A., Munoz-Valencia, A., & Bonilla-Escobar, F. J. (2022). War on Ukraine: impact on Ukrainian medical students. Int J Med Stud, 1, 15–17. Doi:10.5195/ijms.2022.1468.
Sydorova, N. M., Druz, O. V., Savytskyi, V. L., Chernenko, I. A., & Sydorova, L. L. (2022). Primary and secondary prevention of cardiovascular pathology in injured with combat trauma. World of Medicine and Biology, 1(79), 130–134. Doi 10.26724/2079-8334-2022-1-79-130-134.
Taha, M. H., Husain, N. E., Nuri Osman Mukhtar, W., & Elhassan Abdalla, M. (2023). Consolidating Medical Education in Sudan During War. Sudan Journal of Medical Sciences (SJMS), 18(3), 402–412. https://doi.org/10.18502/sjms.v18i3.14093.
Vasianovych, I., Тatarina, O., Lenha, E., Ruda, O., Vainahii, O., & Dymar, N. (2023). Analysis of the effectiveness of the implementation of digital technologies in the educational process of medical HEIs: challenges, optimization. Revista Eduweb, 17(2), 32–42. https://doi.org/10.46502/issn.1856-7576/2023.17.02.3.