Lietuvos chirurgija ISSN 1392–0995 eISSN 1648–9942
2025, vol. 24(3), pp. 227–231 DOI: https://doi.org/10.15388/LietChirur.2025.24(3).7
Case of the Divergent Fallopian Tube: A Rare Cause of Intestinal Obstruction
Mehul Kohli
Armed Forces Medical College, Department of General Surgery, Pune, Maharashtra, India
E-mail: bornfree.mehul@gmail.com
https://orcid.org/0009-0009-3558-1347
https://ror.org/05g6w6j42
Shrey Kansal
Armed Forces Medical College, Department of General Surgery, Pune, Maharashtra, India
E-mail: kansal.shrey23@gmail.com
https://orcid.org/0000-0002-2761-2774
https://ror.org/05g6w6j42
Muthamizh Selvan
Armed Forces Medical College, Department of General Surgery, Pune, Maharashtra, India
E-mail: muthamizh44@gmail.com
https://orcid.org/0009-0008-8499-4343
https://ror.org/05g6w6j42
Jafar Husain
Armed Forces Medical College, Department of General Surgery, Pune, Maharashtra, India
E-mail: jafarhusain@gmail.com
https://orcid.org/0000-0003-2400-1473
https://ror.org/05g6w6j42
Abstract. Background. Intestinal obstruction is a common surgical emergency with diverse etiologies. While adhesions, hernias, and malignancies are frequently implicated, rare anatomical anomalies can occasionally be the cause. Methods. We report a case of a 66-year-old female who presented with complete obstipation for three days. Radiological evaluation revealed dilated bowel loops with a transition point at the distal ileum. Biochemical investigations were notable for metabolic acidosis. Results. Intraoperatively, an anomalous right-sided fallopian tube was identified obstructing the distal ileum, approximately 7 cm proximal to the ileocecal junction. The fallopian tube was resected (salpingectomy). Due to t hinning and impending perforation of the distal ileum, a diversion ileostomy with a distal mucous fistula was performed. Conclusion. This case highlights an unusual cause of small bowel obstruction and emphasizes the importance of considering rare anatomical anomalies in the differential diagnosis of intestinal obstruction.
Keywords: intestinal obstruction, fallopian tube anomaly, salpingectomy, diversion ileostomy.
Received: 2025-05-12. Accepted: 2025-05-31.
Copyright © 2025 Mehul Kohli, Shrey Kansal, Muthamizh Selvan, Jafar Husain. Published by Vilnius University Press. This is an Open Access article distributed under the terms of the Creative Commons Attribution Licence, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction
Small bowel obstruction (SBO) is a common emergency encountered in surgical practice, attributed most commonly to post-operative adhesions, internal hernias, or malignancies. Congenital and acquired anatomical anomalies as causes of obstruction are rare and can present diagnostic and therapeutic challenges [1‒5]. We present a unique case of SBO secondary to a “divergent” right-sided fallopian tube leading to ileal obstruction, an entity rarely reported previously in surgical literature.
Case Report
A 66-year-old postmenopausal lady with no known comorbidities presented with a seven days history of sudden onset intermittent periumbilical pain which gradually involved all quadrants. She also gave history of complete obstipation with minimal oral intake and abdominal distension for three days. The lady did not give any significant history of similar episodes of pain abdomen, recent history of weight loss, melena, altered bowel habits or any previous surgeries.
On examination, she was conscious, oriented and emaciated, weighing 37 kg (BMI: 15 kg/m²). Her vitals were unremarkable except the presence of tachycardia (pulse: 108/min). Abdominal examination revealed distension (diameter: 68 cm), periumbilical tenderness, no palpable lump and exaggerated bowel sounds. Digital rectal examination revealed glove stained with liquid stool and no growth.
Routine laboratory investigations were unremarkable except for ABG which was suggestive of metabolic acidosis. Erect Abdominal X-ray showed multiple air-fluid levels with dilated bowel loops and absence of rectal gas shadow, indicative of mechanical obstruction (Figure 1).
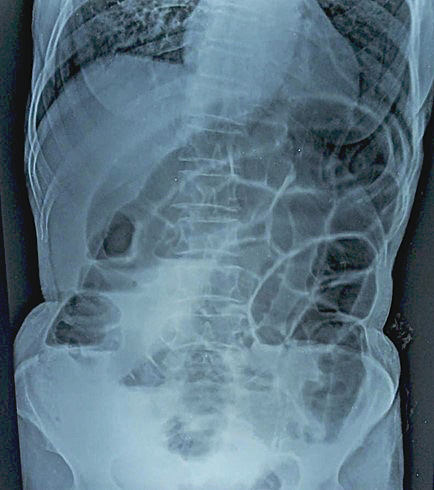
Figure 1. Erect Abdominal X-ray showed multiple air-fluid levels with dilated bowel loops
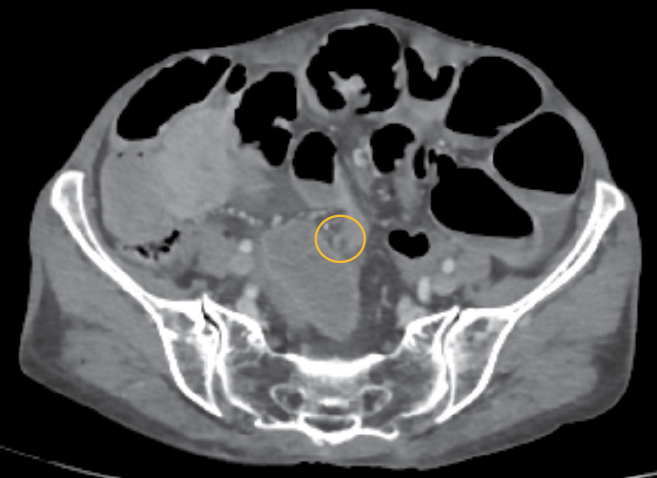
Figure 2. CECT Abdomen & Pelvis showing transition point at the level of distal ileum
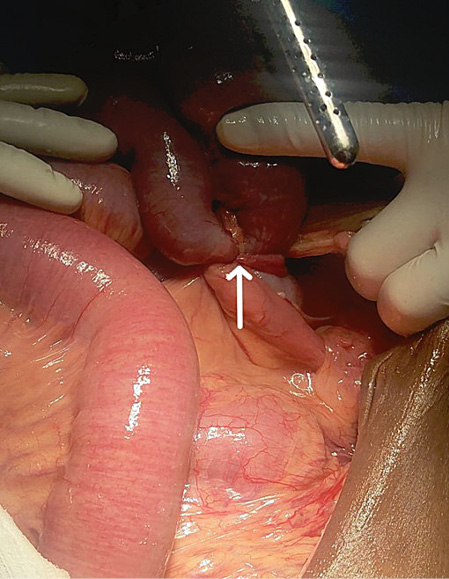
Figure 3. Intra-operative photo showing anomalous right sided fallopian tube compressing distal ileum
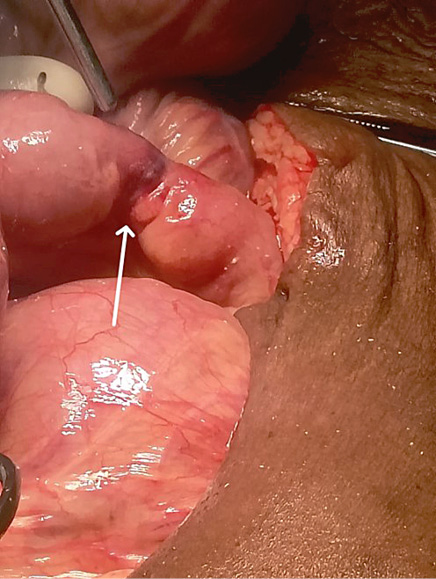
Figure 4. Intra-operative photo showing transition zone (dilated proximal bowel loops) post salpingectomy
Contrast Enhanced Computed Tomography (CECT Abdomen & Pelvis) was suggestive of acute intestinal obstruction with possible transition point in distal ileum (approx. 10 cm from ileo colic junction) with bowel loops showing normal enhancement pattern and no evidence of perforation. Free fluid was noted in the peri-hepatic, peri splenic, hepato renal pouch inter bowel space and pelvis (Figure 2).
The patient was initially resuscitated with intravenous fluids, nasogastric decompression and antibiotics. Given the history of persistence of symptoms for nearly seven days, the patient was taken up for an emergency exploratory laparotomy.
Intraoperatively, proximal small bowel loops were dilated with an anomalous right-sided fallopian tube compressing the distal ileum approximately 7 cm from the ileocecal junction (Figure 3), forming a transition point (Figure 4). The ileal segment was thinned out with impending perforation (Figure 5). Right salpingectomy was done to relieve the obstruction. Dilated proximal bowel loops were decompressed and diversion ileostomy was made from the thinned out segment with a distal mucous fistula.
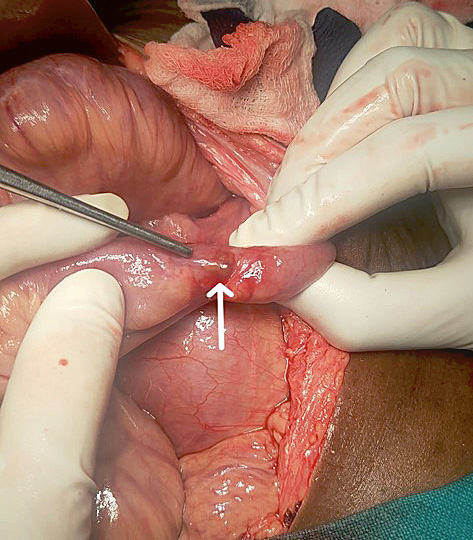
Figure 5. Intra-operative photo showing thinned out ileal segment with impending perforation
Postoperatively, the patient was shifted to Surgical ICU on mechanical ventilation and ionotropic support. On post-operative day 2, the patient was extubated. She was started on nasogatric feed from post-operative day 3 and on soft diet from post-operative day 5. Patient was discharged on post-operative day 7 with a functioning stoma.
Discussion
SBO in the elderly can be most commonly encountered due to post-operative adhesions, internal hernias, intestinal tuberculosis and malignancies [6]. Fallopian tube-related pathologies are well-documented in gynaecological disorders, its role in mechanical small bowel obstruction is exceedingly rare as was noted in our case.
Cameron et al. [7] previously described a case of SBO due to an internal hernia through the broad ligament with the fallopian tube wrapped around the bowel in which the patient had undergone multiple gynaecological surgeries in the past. This was not the case in our patient as she had not undergone any prior surgery.
Choi et al. [8] described the ectopic location of the fallopian tube due to torsion of the fallopian tube which further lead to the small bowel obstruction. In our patient, the “divergent” right fallopian tube occurring in a postmenopausal lady did not undergo torsion. The aberrant fallopian tube occurred even in the absence of any anatomical abnormality.
This case highlights the importance of considering uncommon etiologies in elderly patients presenting with small bowel obstruction. A thorough intraoperative assessment and a high index of suspicion for rare anatomical variants can aid in timely intervention.
Conclusion
This case illustrates an extremely rare cause of mechanical intestinal obstruction in an elderly lady without any predisposing factors. Clinicians should remain vigilant for uncommon anatomical anomalies when evaluating patients with intestinal obstruction as early recognition of signs and appropriate surgical management can significantly improve patient outcomes.
Conflict of Interest
None declared.
Funding
None received.
References
1. Chen XZ, Wei T, Jiang K, Yang K, Zhang B, Chen ZX, Chen JP, Hu JK. Etiological factors and mortality of acute intestinal obstruction: a review of 705 cases. Zhong Xi Yi Jie He Xue Bao 2008; 6(10): 1010–1016.
2. McEntee G, Pender D, Mulvin D, McCullough M, Naeeder S, Farah S, Badurdeen MS, Ferraro V, Cham C, Gillham N, Matthews P. Current spectrum of intestinal obstruction. Br J Surg 2005; 74(11): 976–980.
3. Menzies D, Parker M, Hoare R, Knight A. Small bowel obstruction due to postoperative adhesions: treatment patterns and associated costs in 110 hospital admissions. Ann R Coll Surg Engl 2001; 83(1): 40–46.
4. Madziga AG, Nuhu AI. Causes and treatment outcome of mechanical bowel obstruction in north eastern Nigeria. West Afr J Med 2008; 27(2): 101–105.
5. Cox MR, Gunn IF, Eastman MC, Hunt RF, Heinz AW. The operative aetiology and types of adhesions causing small bowel obstruction. Aust N Z J Surg 1993; 63(11): 848–852.
6. Hayanga AJ, Bass-Wilkins K, Bulkley GB. Current management of small-bowel obstruction. Adv Surg 2005; 39: 1–33.
7. Cameron M, Janakan G, Birch D, Nazir S. A closed loop obstruction caused by entrapment of the fallopian tube and herniation through the broad ligament. Int J Surg Case Rep 2015; 12: 57–59.
8. Choi HN, Arafat Y, Lucky T, Dharmawardhane A. A unique case of small bowel obstruction secondary to internal hernation due to a torted fallopian tube adherent to the sigmoid colon. Int J Case Rep Images 2019; 10: 101069Z01CN2019.