Lietuvos chirurgija ISSN 1392–0995 eISSN 1648–9942
2025, vol. 24(4), pp. 320–324 DOI: https://doi.org/10.15388/LietChirur.2025.24(4).9
An Ileo-ceco-colo-colic Intussusception in a 12-Year-Old Female: A Case Report and Review of the Literature
Parth Vaghela
GCS Medical College, Hospital and Research Centre, Department of Cardiothoracic
and Vascular Surgery, Ahmedabad, Gujarat, India
E-mail: parth_vaghela911@yahoo.com
https://orcid.org/0000-0003-3688-6096
Maya Damor
GCS Medical College, Hospital and Research Centre, Department of Anaesthesia,
Ahmedabad, Gujarat, India
E-mail: drmayadamor25@yahoo.com
https://orcid.org/0009-0009-2212-0074
Abstract. Introduction. Intussusception is a leading cause of acute intestinal obstruction in young children, most commonly occurring between 6 months and 2 years of age. However, it becomes increasingly rare in older pediatric populations and often presents with atypical features. Among the uncommon variants, ileo-ceco-colo-colic intussusception – where the terminal ileum, cecum, and segments of the colon invaginate into the distal colon – represents an extremely rare and complex entity. Prompt recognition and timely intervention are essential to prevent complications such as bowel ischemia and necrosis. Case presentation. We present the case of a 12-year-old previously healthy female who arrived at the emergency department with acute onset abdominal pain, bilious vomiting, and rectal bleeding. Abdominal ultrasound and contrast-enhanced CT scan revealed a long-segment intussusception involving the terminal ileum, cecum, ascending colon, and extending into the transverse colon. Attempts at non-operative (pneumatic) reduction were unsuccessful. Due to clinical signs of peritonism and suspected bowel ischemia, an emergency exploratory laparotomy was performed. Intraoperative findings confirmed a non-reducible intussusception with segments of non-viable bowel. A right hemicolectomy with primary ileocolic anastomosis was carried out. Histopathological analysis demonstrated hypertrophied Peyer’s patches as a possible lead point, without evidence of malignancy or other pathological lesions. Conclusions. This case illustrates a rare and advanced form of intussusception in an older pediatric patient. Given its atypical presentation and increased likelihood of underlying pathology, older children with suspected intussusception warrant thorough evaluation and early surgical consideration. This report emphasizes the importance of maintaining a high index of suspicion, utilizing appropriate imaging modalities, and pursuing timely surgical management when non-operative reduction fails or complications arise.
Keywords: intussusception, ileo-ceco-colo-colic intussusception, paediatric bowel obstruction, rare intussusception variants, right hemicolectomy.
Received: 2025-07-04. Accepted: 2025-09-01.
Copyright © 2025 Parth Vaghela, Maya Damor. Published by Vilnius University Press. This is an Open Access article distributed under the terms of the Creative Commons Attribution Licence, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction
Intussusception, the invagination of one segment of the intestine into another, is the most common cause of intestinal obstruction in infants and young children but becomes increasingly rare beyond the age of five. The typical presentation involves ileo-colic intussusception; however, ileo-ceco-colo-colic variants, where the terminal ileum, cecum, and portions of the ascending and transverse colon invaginate into the distal colon, are extremely rare, particularly in older children.
This report presents a rare case of ileo-ceco-colo-colic intussusception in a 12-year-old girl, outlining clinical presentation, diagnosis, management, and a literature-based discussion.
Case Presentation
A 12-year-old previously healthy female presented to the emergency department with a 24-hour history of colicky abdominal pain, non-bilious vomiting, and passage of “red currant jelly” stool. There was no previous similar history, trauma, or known gastrointestinal disease.
Vital signs: HR ‒ 110 bpm, BP ‒ 100/60 mmHg, temperature ‒ 37.5 °C.
Physical examination: soft, diffusely tender abdomen with a palpable, sausage-shaped mass in the right upper quadrant.
Laboratory findings: mild leucocytosis (WBC 13,500/mm³), normal haemoglobin and serum electrolytes.
Imaging
• Ultrasound revealed a target sign extending unusually far into the left abdomen.
• Contrast-enhanced CT confirmed a long-segment intussusception involving the terminal ileum, cecum, ascending colon, and transverse colon ‒ consistent with ileo-ceco-colo-colic intussusception.
Management
The patient underwent emergency laparotomy. Intraoperative findings confirmed the imaging diagnosis (Figure 1). Manual reduction was partially successful. Due to ischemic Gangrenous changes (Figure 2) and segmental thickening of the right colon, a right hemicolectomy with primary anastomosis was performed.

Figure 1. Intraoperative intusucception evaluation
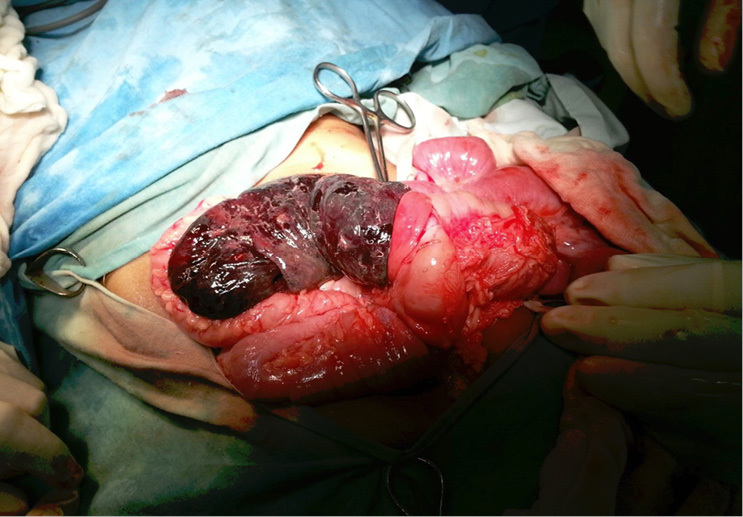
Figure 2. Gangrenous bowel loops
Histopathology
Showed no malignancy; hypertrophied lymphoid follicles (Peyer’s patches) in the ileum and cecum were noted ‒ suggesting a possible lead point in the context of a viral illness.
Post-operative course
Uneventful. The patient was discharged on postoperative day 6 and remained well at 6-month follow-up.
Discussion
Intussusception remains the most common cause of intestinal obstruction in infants and toddlers, but its incidence markedly decreases with age. In older children, particularly those over six years, intussusception is not only rare but often associated with atypical presentations and an increased likelihood of a pathological lead point [1]. The classical form ileo-colic is commonly encountered, but more complex variants such as ileo-ceco-colo-colic intussusception are exceedingly rare, especially in the paediatric population. In this condition, the terminal ileum, cecum, and ascending colon invaginate further into the transverse or descending colon, resulting in a long-segment telescoping of bowel that poses diagnostic and therapeutic challenges [2, 3]. In the case presented, the extent of bowel involvement and the age of the patient made the condition particularly unusual. In such presentations, the possibility of a pathological lead point, such as Meckel’s diverticulum, lymphoma, duplication cysts, or intestinal polyps, must always be considered [4]. However, in our patient, histopathology revealed hypertrophied Peyer’s patches in the terminal ileum and cecum, which may reflect benign lymphoid hyperplasia often seen in post-viral states. Although most intussusceptions in infants are idiopathic, a definitive cause can be identified in up to 75% of older children with atypical forms [5].
Diagnostic imaging plays a crucial role in identifying the type and extent of intussusception. Ultrasound remains the first-line imaging modality due to its high sensitivity (up to 98%) and non-invasive nature [6]. The “target” or “donut” sign is pathognomonic, but in extended variants like ileo-ceco-colo-colic intussusception, sonographic interpretation may be limited by overlapping loops and extensive involvement. In such cases, contrast-enhanced computed tomography (CT) offers a more comprehensive view, delineating the full extent of intussusception and providing additional information about bowel viability, ischemia, or perforation [7]. The initial management of intussusception typically involves non-operative reduction via pneumatic or hydrostatic enema. However, the success of this approach significantly declines in older children and in cases involving complex or long-segment variants. Moreover, signs of peritonitis, hemodynamic instability, or failure of reduction mandate surgical intervention [8]. In the present case, due to the failure of non-operative reduction and signs of ischemia on imaging, the patient underwent exploratory laparotomy. Although partial reduction was achieved intraoperatively, the ischemic appearance of the cecum and ascending colon necessitated a right hemicolectomy with primary anastomosis.
A literature review reveals that ileo-ceco-colo-colic intussusception has been reported only in a handful of paediatric cases worldwide, with the majority requiring surgical intervention. The most common lead points described in these reports include Meckel’s diverticulum, Burkitt lymphoma, and juvenile polyps [2, 4, 9]. The rarity of this variant, coupled with non-specific clinical symptoms, highlights the need for a high index of suspicion, particularly in older children presenting with signs of obstruction and gastrointestinal bleeding. This case emphasizes the importance of recognizing atypical intussusception presentations, particularly in older children. Early imaging with CT, timely surgical intervention, and histopathological evaluation are essential to rule out sinister pathology and to prevent complications such as bowel necrosis, perforation, and sepsis. It also underscores the necessity for clinicians to consider rare anatomical variants in the differential diagnosis, as prompt recognition significantly impacts outcomes.
Declarations
Funding. Not applicable.
Conflict of interest. Not applicable.
Ethics approval. The Institutional Review Board (IRB) or equivalent ethics committee of the GCS Medical College, hospital and research centre, research approval not applicable as this is a case report/study.
Consent for participation. The subject provided informed written consent for the publication of the study data.
Written consent for publication. The subject provided informed written consent for the publication of the study data.
Availability of data and material. The datasets during and/or analysed during the current study available from the corresponding author on reasonable request.
Code availability. Not applicable.
Authors contribution
Dr. Parth Vaghela and dr. Maya Damor have contributed to the conceptuality and design, data collection, data analysis, interpretation of data, drafting the work, revising the work, and approving the final version.
Dr. Parth Vaghela, dr. Maya Damor have contributed to the supervision and approving the final version.
Dr. Maya Damor has contributed to the resources.
References
1. Blakelock R, Beasley SW. The clinical implications of differences between primary and secondary intussusception. Pediatr Surg Int 1998; 13(5‒6): 308–310.
2. Lee YJ, Park KH, Kim YH. A case of ileocecocolic intussusception with a long segment in a 9-year-old girl. J Pediatr Surg 2008; 43(11): e43–e45.
3. Wiersma R, Hadley GP. Ileo-ceco-colo-colic intussusception in a 4-year-old child. Pediatr Radiol 2004; 34(10): 862–864.
4. Stringer MD, Pablot SM, Brereton RJ. Paediatric intussusception: a 10-year review. Br J Surg 1992; 79(9): 867–876.
5. Apelt N, Featherstone N, Giuliani S. Management of intussusception in children: a survey of UK practice. J Pediatr Surg 2013; 48(11): 2274–2278.
6. Hernanz-Schulman M. Infantile intussusception: role of imaging in diagnosis and treatment. Radiology 2003; 226(2): 331–339.
7. Daneman A, Navarro O. Intussusception. Part 1: A review of diagnostic approaches. Pediatr Radiol 2004; 34(2): 95–108.
8. Shouldice M, Fraser G, Barker P. Surgical vs. non-surgical management of pediatric intussusception: a retrospective analysis. World J Surg 2017; 41(3): 712–716.
9. Okuyama H, Yoshida M, Tainaka T. Surgical treatment of a complex intussusception in a child: a case report and review of the literature. Pediatr Surg Int 2015; 31(7): 671–674.