Lietuvos chirurgija ISSN 1392–0995 eISSN 1648–9942
2025, vol. 24(4), pp. 316–319 DOI: https://doi.org/10.15388/LietChirur.2025.24(4).8
Intrathoracic Sewing Needle in an Infant: An Unusual Case of Foreign Body Migration
Neel Aggerwal
Post Graduate Institute of Child Health, Department of Pediatric Surgery, Noida, India
E-mail: aggerwal.pgich@gmail.com
Chandra Vibhash
Post Graduate Institute of Child Health, Department of Pediatric Surgery, Noida, India
E-mail: chandravibhash@yahoo.com
Pragya Mishra
Post Graduate Institute of Child Health, Department of Pediatric Surgery, Noida, India
E-mail: tinytots2417@gmail.com
Umesh B. Singh
Post Graduate Institute of Child Health, Department of Pediatric Surgery, Noida, India
E-mail: singhub.2008@gmail.com
Abstract. Foreign body incidents are common in children, primarily involving ingestion or inhalation. However, transcutaneous migration of sharp objects like sewing needles into the thoracic cavity is exceptionally rare and potentially dangerous. We report a unique case of an intrathoracic sewing needle in a six-month-old infant, highlighting the diagnostic challenges, imaging findings, surgical approach, and the clinical outcome.
Keywords: sewing needle, chest, migration.
Received: 2025-08-03. Accepted: 2025-08-29.
Copyright © 2025 Neel Aggerwal, Chandra Vibhash, Pragya Mishra, Umesh B. Singh. Published by Vilnius University Press. This is an Open Access article distributed under the terms of the Creative Commons Attribution Licence, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction
Foreign bodies have been reported in nearly every anatomical region, especially in children who are naturally inquisitive. Thoracic foreign bodies in pediatric patients typically arise from aspiration or ingestion. Penetrating chest injuries in infants are uncommon, with very few reports of sewing needle migration into the thorax [1].
Such incidents may be accidental or intentional, although most published cases describe adult presentations or involve other regions like the abdomen, cranium, or heart [2]. This case underscores the importance of clinical suspicion and thorough evaluation when no trauma history is evident.
Case report
A six-month-old female infant initially presented to the hospital with a two-day history of fever but no respiratory complaints. She was investigated and advised medications. Two days later, she returned with tachypnea. On examination, her respiratory rate was 48/min with a SpO₂ of 94% on 2 L/min oxygen via nasal prongs, but stable. Chest radiograph revealed a linear, radiopaque foreign body suggestive of a needle (Figure 1). The direction of needle was almost horizontal and not in the line with the trachea-bronchial tree. There was no history of trauma, insertion, or ingestion reported by caregivers. Physical examination revealed no external wound, swelling, or inflammation, and the needle was not palpable.
Contrast-enhanced CT of the chest confirmed a 3–4 cm metallic foreign body in the right paraspinal intrathoracic area, crossing the 7th intercostal space, associated with right lower lobe consolidation and mild pleural effusion (Figure 1).
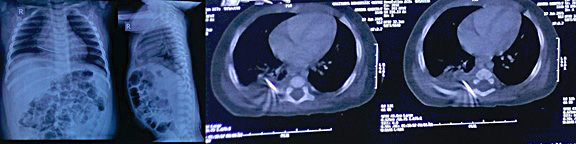
Figure 1. Chest X-rays and CECT chest at the time of admission
The plan for extraction was to explore from posterior chest muscular plane with minimal open thoracotomy/VATS if not retrieved. The patient underwent surgical exploration in the prone position. The needle was marked using serial intraoperative X-rays and a transverse incision was made over the marked site. No subcutaneous erythema was detected and a sewing needle was successfully retrieved from the muscle plane where it was embedded 1 cm deep just above intercoastal muscle passing longitudinally into thorax, which was removed completely with no breakage (Figure 2). The postoperative course was uneventful, and the infant was discharged after 48 hours and has been asymptomatic on follow up.

Figure 2. Intraoperative X-rays, retrieved sewing needle from back
Discussion
Intrapulmonary sewing needles are relatively rare in clinical practice. Four entry routes have been detailed in literature: transbronchial, transesophageal, hematogenous and transcutaneous [3]. Sharp thoracic foreign bodies in pediatric patients are predominantly due to aspiration. Foreign body penetration can also be due to accident/self-injury/abuse [4]. Transcutaneous migration is extremely rare, especially in infants, and often goes unnoticed due to absent or subtle symptoms [5]. The clinical presentation is variable, depending on the site, depth, and trajectory of the object.
In our case, there was no reported trauma or indication of abuse. The likely scenario is accidental transcutaneous penetration during routine activities like crawling, possibly due to unnoticed objects embedded in fabrics or bedding. Similar mechanisms have been suggested in previous literature, particularly in settings where infants are tightly wrapped [5].
Migration of sharp objects can result in significant complications, including pneumothorax, hemothorax, infection, or injury to vital structures like the heart or major vessels [6]. Hence, early identification and removal are crucial.
Radiological imaging is indispensable for localization. While chest radiography is useful for initial detection, computed tomography provides superior anatomical detail, aiding surgical planning. Intraoperative localization can be challenging due to potential migration [1]. Techniques such as fluoroscopy, ultrasound, and serial radiographs have been employed, as in our case, to successfully guide removal.
Surgical options vary depending on the object’s location. While video-assisted thoracoscopic surgery (VATS) offers a minimally invasive alternative, open exploration remains reliable in selected cases, particularly when the object is superficially located in the chest wall [1].
To the best of our knowledge, very few cases of transcutaneous migrated intrapulmonary needle in foreign body in infants have been reported till date, out of which majority needed VATS or thoracotomy, and in only few cases needle was retrieved without entering thorax.
Conclusion
Penetrating thoracic injuries by sewing needles are exceedingly rare in infants. High clinical suspicion, appropriate imaging, and timely surgical intervention are essential to avoid complications. Surgeons should be aware of the migratory potential of such objects and the role of intraoperative imaging to ensure safe and effective retrieval.
Author contribution
Dr. Neel Aggerwal ‒ conceptualization, investigations, writing original draft.
Dr. Chandra Vibhash ‒ conceptualization, writing original draft.
Dr. Pragya Mishra ‒ investigations, writing review and editing.
Dr. Umesh B. Singh ‒ visualization, writing review and editing.
References
1. Gebreselassie HA, Godu BG, Erge MG. Migratory foreign body in the chest. J Pediatr Surg Case Rep 2021; 74: 102050.
2. Uguralp S, Harma B, Karaman A. Intrathoracic sewing needle: an unusual penetrating injury in two children. J Inonu Univ Med Fac 2009; 16(2): 121–123.
3. Motohiro A, Hiroto N, Takada S, Ando K. Surgically removed intrathoracic needle: a report of three cases. J Jpn Assoc Chest Surg 1993; 7: 685‒688.
4. Bakal U, Tartar T, Kazez A. A rare mode of entry for needles observed in the abdomen of children: penetration. J Indian Assoc Pediatr Surg 2012; 17(3): 130–131.
5. Jyoti B, Kumar AN, Harish J. Transcutaneous migration of foreign body into thorax in children: a report of two cases. J Pediatr Surg Case Rep 2016; 14: 32–34.
6. Akcam Tİ, Cakan A, Ergonul AG, Erol Y, Cagırıcı U. Removal of a foreign body from the chest wall guided by fluoroscopy. Ege J Med 2013; 52: 208–210.