Lietuvos chirurgija ISSN 1392–0995 eISSN 1648–9942
2026, vol. 25(1), pp. 46–56 DOI: https://doi.org/10.15388/LietChirur.2026.25(1).4
Endoscopic Retrograde Cholangiopancreatography Followed by Laparoscopic Cholecystectomy Versus Laparoscopic Common Bile Duct Exploration with Cholecystectomy: Comparative Outcomes and Predictive Models for Choledocholithiasis
Mohamed Tag El-Din Mohamed Sayed
Sohag University, Department of General Surgery, Sohag, Egypt
E-mail: mohamedtag987@yahoo.com
https://orcid.org/0009-0004-1520-1451
https://ror.org/02wgx3e98
Abdullah Atyah Ali Abdullah
Luxor University, Department of General Surgery, Luxor, Egypt
E-mail: dr.abodabod100@gmail.com
https://orcid.org/0000-0002-8433-3966
https://ror.org/035hzws46
Nehal Ashraf Zaki Mahmoud
South Valley University, Faculty of Medicine, Department of Medical Biochemistry, Egypt
E-mail: nehal.ashraf888@gmail.com
https://orcid.org/0000-0002-4917-1834
https://ror.org/00jxshx33
Abstract. Background. Choledocholithiasis can be treated by a two-stage approach – endoscopic retrograde cholangiopancreatography followed by laparoscopic cholecystectomy (ERCP+LC) – or a single-stage approach using laparoscopic common bile duct exploration with cholecystectomy (LCBDE+LC). Comparative evidence on perioperative outcomes and predictive modeling remains limited. Methods. This prospective observational study included 200 adults with gallbladder and CBD stones managed at a tertiary center (100 ERCP+LC, 100 LCBDE+LC). Standardized protocols guided preoperative assessment, interventions, and discharge. Primary outcome was successful CBD stone clearance with completion of cholecystectomy. Secondary outcomes included operative time, hospital stay, pain scores (VAS at 24 h and 3 days), complications, retained stones, and satisfaction. Logistic regression models predicted retained stones and complications; performance was assessed by ROC-AUC, Brier score, and calibration. Nomograms and an integrated risk score table were developed. Results. LCBDE patients had larger CBD diameters (13.18±2.01 mm vs. 10.94±2.46 mm) and stones (6.29±1.47 mm vs. 5.65±1.69 mm). Operative time and hospital stay were similar. Pain at 24 h was lower in LCBDE (median 5 [IQR 5–6]) vs. ERCP+LC (6 [6–7]; p < 0.001), equalizing by day 3. Postoperative direct bilirubin was lower after ERCP+LC (p = 0.036). Complications were infrequent; retained stones occurred in 1% vs. 3%. Predictive models showed AUC 0.92 for retained stones and 0.73 for complications. Nomograms and a points table enable bedside risk stratification. Conclusions. Both strategies are safe and effective. LCBDE offers lower early pain and suits high stone burden; ERCP+LC remains appropriate for urgent decompression or limited laparoscopic resources. Risk-based tools may support individualized decision-making.
Keywords: choledocholithiasis, ERCP, LCBDE, laparoscopic cholecystectomy, CBD stones, predictive models.
Received: 2025-12-01. Accepted: 2025-12-15.
Copyright © 2026 Mohamed Tag El-Din Mohamed Sayed, Abdullah Atyah Ali Abdullah, Nehal Ashraf Zaki Mahmoud. Published by Vilnius University Press. This is an Open Access article distributed under the terms of the Creative Commons Attribution Licence, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction
Common bile duct (CBD) stones occur in 10–20% of patients with gallstones and represent a major cause of biliary obstruction worldwide [1]. Untreated choledocholithiasis can lead to severe complications such as cholangitis, obstructive jaundice, and pancreatitis, which carry significant morbidity and mortality [2]. Over the past decade, management strategies have shifted toward minimally invasive approaches, aiming to reduce complications and hospital stay while maintaining high stone clearance rates [3].
Endoscopic retrograde cholangiopancreatography (ERCP) remains the most widely used first-line treatment for CBD stones, offering high success rates for duct clearance [4]. However, ERCP is associated with risks such as post-procedural pancreatitis, bleeding, and long-term sphincter dysfunction [5]. These limitations have driven interest in laparoscopic common bile duct exploration (LCBDE), which enables single-stage management of gallbladder and CBD stones during laparoscopic cholecystectomy [6].
Recent meta-analyses and randomized trials suggest that LCBDE provides comparable or superior stone clearance compared to ERCP, particularly for large or multiple stones, while reducing the need for multiple interventions and shortening hospital stay [7, 8]. Technological advances, including high-definition choledochoscopy and laser lithotripsy, have further improved the safety and feasibility of LCBDE [9]. Updated guidelines emphasize individualized treatment based on patient comorbidities, stone characteristics, and institutional expertise [10].
Despite these developments, controversy persists regarding the optimal approach, especially in resource-limited settings and for complex stones. High-quality comparative studies focusing on perioperative outcomes, complications, and patient satisfaction are essential to guide evidence-based practice [11].
This study compares ERCP followed by laparoscopic cholecystectomy (ERCP+LC) versus laparoscopic common bile duct exploration with cholecystectomy (LCBDE) in patients with choledocholithiasis, analyzing operative parameters, postoperative outcomes, and patient-reported satisfaction.
Methods
Study design and ethics. This was a prospective comparative observational study conducted at a single tertiary center between January 2018 and December 2024. All patients were managed according to standardized institutional protocols for choledocholithiasis. Ethical approval was obtained from the Sohag University ethical committee (January 2018) in accordance with the Declaration of Helsinki, and patient confidentiality was maintained throughout the study.
The extended study period reflects the relatively low annual case load and the strict inclusion criteria applied to ensure homogeneity.
Participants. We included adult patients (≥18 years) with gallbladder stones and radiological or clinical evidence of common bile duct (CBD) stones.
Exclusion criteria: acute cholecystitis, acute pancreatitis, irreversible coagulopathy, end-stage organ failure, cirrhosis, intrahepatic biliary disease, liver masses, recurrent CBD stones, or malignant biliary/pancreatic tumors.
Preoperative assessment. All patients underwent routine laboratory tests (complete blood count, liver function tests, coagulation profile, pancreatic enzymes) and imaging. Abdominal ultrasound was performed in all cases, and magnetic resonance cholangiopancreatography (MRCP) was used to confirm CBD stone number, size, and duct anatomy.
Interventions. LCBDE group. Patients underwent laparoscopic cholecystectomy with CBD exploration during the same operation. Stones were extracted via a transcystic approach when feasible or by choledochotomy for large or impacted stones. CBD closure was performed primarily or over a T-tube based on intraoperative findings.
ERCP+LC group. Patients first underwent ERCP for CBD stone clearance, followed by laparoscopic cholecystectomy during the same admission (target ≤72 hours). Reasons for any delay were documented.
All procedures were performed by consultant surgeons with equivalent experience in laparoscopic biliary surgery. Operative techniques and perioperative care pathways were standardized across the study period.
Perioperative management and discharge criteria. Postoperative care included standardized analgesia, early mobilization, and monitoring. Oral intake was resumed after bowel function returned. Discharge required stable vital signs, adequate pain control with oral medications, tolerance of diet, improving liver tests, and absence of bile leak or retained stones. Imaging before discharge was performed when clinically indicated.
Outcome measures. Primary outcome. Successful clearance of CBD stones with completion of cholecystectomy without conversion. Clearance was confirmed intraoperatively by cholangiography or endoscopic visualization.
Secondary outcomes. Operative time, intraoperative complications, conversion rates, postoperative pain scores (VAS at 24 h and 3 days), hospital stay, postoperative complications (Clavien–Dindo ≥II), retained stones within 6 months, and patient satisfaction at discharge.
Sample size. Of 209 screened patients, 200 were included (100 per group). Sample size was based on prior institutional data suggesting a 15% difference in clearance rates between approaches. With α = 0.05 and 80% power, at least 90 patients per group were required; this was increased to 100 to account for potential loss to follow-up.
Statistical analysis. Analyses followed an intention-to-treat principle. Continuous variables were compared using Welch’s t-test or Mann–Whitney U as appropriate; categorical variables using χ² or Fisher’s exact test. Logistic regression was used to identify predictors of postoperative complications and retained stones.
Adjusted comparisons employed ANCOVA controlling for age, diabetes, CBD diameter, and stone size. Model assumptions were verified. Missing data were handled using multiple imputation by chained equations.
Predictive modeling included logistic regression with nomogram development. Model performance was assessed using ROC-AUC, Brier score, and calibration plots.
All analyses were conducted using Python (pandas, statsmodels) and SPSS v29.0; significance was set at p < 0.05.
Results
Demographics and clinical characteristics. A total of 200 patients were analyzed, divided equally between the ERCP+LC group (n = 100) and the LCBDE group (n = 100). The mean age was comparable between groups (41.5±9.5 vs. 43.4±12.6 years). Females constituted 68 patients (68%) in ERCP+LC and 59 patients (59%) in LCBDE. Comorbidities were present in 38 patients (38%) in each group, with diabetes being more frequent in the LCBDE group (21 patients, 21%) compared to ERCP+LC (12 patients, 12%) (Table 1).
Operative details and stone characteristics. Operative time was similar between groups (140.6±44.2 vs. 138.3±20.4 min). Length of hospital stay showed no significant difference (7.2±2.3 vs. 6.8±2.1 days). However, CBD diameter and stone size were significantly larger in the LCBDE group (13.2±2.0 mm vs. 10.9±2.5 mm; 6.3±1.5 mm vs. 5.6±1.7 mm, respectively) (Table 2).
Table 1. Demographics and clinical data
|
Variable |
ERCP+LC |
LCBDE |
|---|---|---|
|
Age (years) |
41.52±9.54 |
43.42±12.63 |
|
Gender |
Female: 68 (68%) |
Female: 59 (59%) |
|
Male: 32 (32%) |
Male: 41 (41%) |
|
|
Comorbidities |
None: 62% |
None: 62% |
|
Hypertensive: 15% |
Hypertensive: 9% |
|
|
Diabetic: 12% |
Diabetic: 21% |
|
|
Both: 11% |
Both: 8% |
Table 2. Operative details and stone features
|
Variable |
ERCP+LC |
LCBDE |
|---|---|---|
|
Operative time (min) |
140.65±44.21 |
138.30±20.40 |
|
Length of stay (days) |
7.18±2.28 |
6.79±2.09 |
|
CBD diameter (mm) |
10.94±2.46 |
13.18±2.01 |
|
Stone size (mm) |
5.65±1.69 |
6.29±1.47 |
|
Number of stones |
Single: 90% |
Single: 92% |
|
Site of stone |
Distal: 62% |
Distal: 74% |
Laboratory parameters. Preoperative bilirubin levels were similar between groups. Postoperative total and direct bilirubin decreased in both groups, with a slightly greater reduction in ERCP+LC. Postoperative direct bilirubin was significantly lower in ERCP+LC (0.83±0.62 vs. 1.01±0.58 mg/dL; p = 0.036) (Table 3).
Table 3. Pre- and postoperative bilirubin levels
|
Variable |
ERCP+LC |
LCBDE |
|---|---|---|
|
Preoperative total bilirubin |
2.77±1.55 |
2.80±1.36 |
|
Preoperative direct bilirubin |
2.26±1.49 |
2.33±1.28 |
|
Postoperative total bilirubin |
1.23±0.68 |
1.39±0.58 |
|
Postoperative direct bilirubin |
0.83±0.62 |
1.01±0.58 |
Postoperative outcomes. Pain scores at 24 hours were significantly lower in LCBDE (median 5 [IQR 5–6]) compared to ERCP+LC (median 6 [IQR 6–7]; p < 0.001), while pain at 3 days was similar. Postoperative complications occurred in 8% of ERCP+LC and 7% of LCBDE patients, with wound infection and pancreatitis being the most common. Conversion rates were identical (3%), and retained CBD stones were rare (1% vs. 3%) (Table 4).
Comparative analysis. Statistical comparison confirmed significant differences in CBD diameter (mean difference −2.24; 95% CI −2.87 to −1.61), stone size (−0.64; 95% CI −1.08 to −0.20), and postoperative direct bilirubin (−0.18; 95% CI −0.35 to −0.01), favoring ERCP+LC for biochemical recovery and LCBDE for larger stones. Pain at 24 hours was significantly lower in LCBDE (median 5 [IQR 5–6] vs. 6 [IQR 6–7]; Mann–Whitney U; p < 0.001) (Table 5).
Table 4. Postoperative outcomes
|
Outcome |
ERCP+LC |
LCBDE |
|---|---|---|
|
Pain at 24 h (median [IQR]) |
6 [6–7] |
5 [5–6] |
|
Pain at 3 days (median [IQR]) |
1 [1–2] |
1 [1–2] |
|
Postoperative complications |
None: 92% |
None: 93% |
|
Conversion to other procedure |
3% |
3% |
|
Retained CBD stone |
1% |
3% |
|
Satisfaction score |
High: 75% |
High: 78% |
Table 5. Comparative analysis between groups
|
Variable |
ERCP+LC (mean±SD) |
LCBDE (mean±SD) |
Mean difference (95% CI) |
p-value |
|---|---|---|---|---|
|
CBD diameter |
10.94±2.46 |
13.18±2.01 |
−2.24 |
<0.001 |
|
Stone size |
5.65±1.69 |
6.29±1.47 |
−0.64 |
0.005 |
|
Postoperative direct bilirubin |
0.83±0.62 |
1.01±0.58 |
−0.18 |
0.036 |
|
Pain at 24 h |
6 [6–7] |
5 [5–6] |
Mann‒Whitney U |
<0.001 |
Multivariate analysis. Logistic regression did not identify statistically significant predictors for retained CBD stones or postoperative complications. However, comorbidity and LCBDE group showed a trend toward higher odds for retained stones (OR 6.19 and 5.39), while multiple stones increased the odds of complications (OR 6.74) (Table 6; Figure 1). Figure 1 illustrates the forest plot summarizing odds ratios and confidence intervals for both models.
Table 6. Multivariate logistic regression
Predictors of retained CBD stone
|
Predictor |
OR |
95% CI |
p-value |
|---|---|---|---|
|
Comorbidity (any) |
6.19 |
(0.57, 66.98) |
0.134 |
|
Group (LCBDE) |
5.39 |
(0.24, 119.53) |
0.287 |
Predictors of postoperative complications
|
Predictor |
OR |
95% CI |
p-value |
|
Multiple stones |
6.74 |
(0.63, 72.09) |
0.114 |
|
Gender (male) |
0.30 |
(0.07, 1.20) |
0.088 |

Figure 1. Combined forest plot
Forest plot showing odds ratios (OR) and 95% confidence intervals for predictors of retained CBD stone (left panel) and postoperative complications (right panel). The red dashed line indicates OR = 1.
Model performance. The retained CBD stone model demonstrated excellent discrimination (AUC = 0.92; 95% CI 0.86–0.96) and good calibration (Brier score = 0.019), while the postoperative complications model showed moderate performance (AUC = 0.73; 95% CI 0.60–0.86; Brier score = 0.065) (Table 7; Figure 2 and Figure 3). Figure 2 shows ROC curves for both models, and Figure 3 displays calibration plots.
Table 7. Model performance
|
Model |
AUC (95% CI) |
Brier score |
|---|---|---|
|
Retained CBD stone |
0.92 (0.86, 0.96) |
0.019 |
|
Postoperative complications |
0.73 (0.60, 0.86) |
0.065 |
Table 8. Integrated risk score table
|
Predictor |
Points |
Points |
|---|---|---|
|
Age |
0 |
0 |
|
Gender (male) |
0.27 |
6.25 |
|
CBD diameter |
0.01 |
0.2 |
|
Size of stone |
0.27 |
0.71 |
|
Multiple stones |
0.17 |
10 |
|
Stone site (multiple segments) |
10 |
1.48 |
|
Comorbidity |
0.83 |
2.18 |
|
Group (LCBDE) |
0.77 |
0.5 |
Point values reflect rescaled logistic regression coefficients. Higher scores indicate greater risk. The scoring system is exploratory and intended to facilitate bedside estimation of relative risk; external validation is required.

Figure 2. ROC curves
Receiver Operating Characteristic (ROC) curves for logistic regression models predicting retained CBD stone (blue line, AUC = 0.92) and postoperative complications (green line, AUC = 0.73). The red dashed line represents the reference line (AUC = 0.50).

Figure 3. Calibration plots
Calibration plots for retained CBD stone model (left) and postoperative complications model (right). The dashed line represents perfect calibration. Brier scores: 0.019 and 0.065, respectively.
Risk visualization. Nomograms were developed for both outcomes to facilitate clinical application. The retained CBD stone nomogram emphasizes comorbidity and surgical approach as key contributors, while the postoperative complications nomogram highlights multiple stones and comorbidity as major risk factors (Figure 4 and 5).
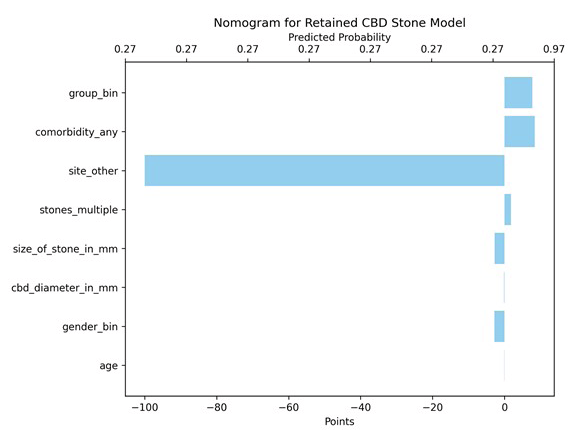
Figure 4. Nomogram for retained CBD stone
Nomogram for predicting retained CBD stone based on logistic regression model. Each predictor contributes points proportional to its coefficient; total points correspond to predicted probability.

Figure 5. Nomogram for postoperative complications
Nomogram for predicting postoperative complications. Multiple stones and comorbidity have the highest impact on risk score.
Integrated risk score. To facilitate clinical application and enable simultaneous assessment of both outcomes, we developed an integrated risk score table (Table 8). This table assigns point values to each predictor using a standardized normalization method, ensuring all values fall within a practical range (0–10). Predictors with the greatest impact on retained CBD stone risk were site of stone (proximal/both), while multiple stones dominated the postoperative complications model. By summing points across predictors, clinicians can estimate relative risk for each outcome and identify patients at higher combined risk. This approach provides a practical framework for bedside decision-making and complements the visual representation offered by the nomograms (Figures 4 and 5). The integrated scoring system highlights how anatomical factors (stone site, CBD diameter) and patient-related factors (comorbidity, stone burden) interact to influence surgical outcomes.
Discussion
Patient selection and stone burden. In our cohort, patients undergoing LCBDE had larger CBD diameters and stones than ERCP+LC (Table 2), reflecting real-world selection of LCBDE for complex burden (large/multiple stones). This agrees with contemporary evidence showing high clearance for LCBDE in large/multiple stones and consolidation into a single-stage pathway [3, 5, 7].
Perioperative efficiency and early recovery. We found similar operative time and length of stay overall (Table 2), while 24-hour pain favored LCBDE and equalized by day 3 (Table 4). Trials and prospective cohorts report that one-stage LCBDE+LC can reduce early discomfort and, in many centers, lower costs relative to two-stage ERCP+LC [5, 6].
Safety profile: pancreatitis vs. bile leak trade-off. Complications were infrequent in both pathways (Table 4). Literature consistently notes higher post-ERCP pancreatitis risk vs. LCBDE, counterbalanced by a bile-leak signal in some LCBDE series ‒ both with low absolute rates when performed by experienced teams [3, 7]. Our low rates of wound infection, bile leak, and retained stones align with those reports.
Biochemical recovery. Post-operative direct bilirubin was lower after ERCP+LC (Table 3) while total bilirubin differences were borderline, a plausible pattern given immediate papillary access and distal stone clearance with ERCP. Updated guidance supports individualized choice based on anatomy/stone complexity and local expertise [4, 10].
Retained stones and conversions. Retained stones were rare (1% vs. 3%), and conversions identical (3%). Large series/meta-analyses show high primary clearance and low residuals across both strategies with consistent use of IOC/choledochoscopy [3, 8, 12].
Pain trajectories and satisfaction. 24-hour pain favored LCBDE, equalizing by day 3, with high satisfaction in both arms (Table 4). Recent comparative work indicates better early comfort and acceptance with single-stage LCBDE, largely by avoiding a staged endoscopic-then-surgical course [6, 7].
Multivariable analysis and model performance. While multivariable models didn’t reach significance ‒ likely due to low event rates ‒ signals for comorbidity (retained stones) and multiple stones (complications) mirror published predictors of adverse outcomes [1, 9]. Our forest plot (Figure 1), ROC (Figure 2), and calibration (Figure 3) show excellent discrimination for retained stones and acceptable for complications, consistent with emerging analytics in CBD stone management [2, 13].
Nomograms and integrated risk score. Our nomograms (Figures 4 and 5) and integrated points table (Table 8) translate coefficients to bedside scoring. They emphasize comorbidity/approach for retained stones and multiple stones/comorbidity for complications ‒ mapping to guideline-driven, patient-centered selection of ERCP+LC vs. LCBDE [4, 10].
Strengths, limitations, and practice implications. Balanced groups (n = 100 each), comprehensive outcomes (including pain/satisfaction), and low residual stones strengthen validity. Limitations include single-center design, potential selection bias (larger stones to LCBDE), and low event rates affecting regression power ‒ issues highlighted by reviews calling for pragmatic RCTs and cost-effectiveness endpoints [8, 11, 13]. Practically, a dual-pathway paradigm emerges: LCBDE for high burden or single-stage priority; ERCP+LC for urgent decompression/poor surgical fitness or limited lap expertise.
Conclusion. Both ERCP followed by laparoscopic cholecystectomy (ERCP+LC) and laparoscopic common bile duct exploration with cholecystectomy (LCBDE+LC) are safe and effective strategies for managing choledocholithiasis. In our cohort, LCBDE was preferentially used for patients with larger CBD diameters and stone sizes and was associated with lower early postoperative pain, while ERCP+LC demonstrated slightly faster biochemical recovery. Overall complication rates, conversion rates, and retained stone incidence were low and comparable between groups.
Although multivariable analysis did not identify statistically significant predictors due to low event rates, trends suggest that comorbidity and stone burden may influence outcomes. The proposed nomograms and integrated risk score table provide practical tools for individualized risk stratification and clinical decision-making. These findings support a dual-pathway approach: LCBDE for high stone burden or when single-stage management is feasible, and ERCP+LC for urgent decompression or in settings with limited laparoscopic expertise. Future multicenter trials should focus on long-term outcomes, cost-effectiveness, and quality-of-life measures to refine treatment algorithms.
Declarations
Funding. This study received no external funding.
Conflicts of interest. The authors declare no competing interests.
Acknowledgements
The authors would like to thank the surgical, anesthesia, and nursing teams at Sohag University Hospital for their continuous support and cooperation throughout this study. The authors also express their gratitude to all participating patients for their valuable contribution.
Author Contributions
Mohamed Tag El-Din Mohamed Sayed ‒ conceptualization, methodology, writing original draft, writing ‒ review and editing.
Abdullah Atyah Ali Abdullah ‒ data curation, writing – review and editing.
Nehal Ashraf Zaki Mahmoud ‒ methodology, data curation, writing ‒ review and editing.
All authors approved the final manuscript.
References
1. Sha Y, Wang Z, Tang R, Wang K, Xu C, Chen G. Modern management of common bile duct stones: Breakthroughs, challenges, and future perspectives. Cureus 2024; 16(12): e75246. DOI: 10.7759/cureus.75246.
2. Wang X, Li Z. Management of common bile duct stones: A comprehensive review. Front Surg 2025; 12: 1658784. DOI: 10.3389/fsurg.2025.1658784.
3. Lan WF, Li JH, Wang QB, Zhan XP, Yang WL, Wang LT, Tang KZ. Comparison of laparoscopic common bile duct exploration and endoscopic retrograde cholangiopancreatography combined with laparoscopic cholecystectomy for patients with gallbladder and common bile duct stones a meta-analysis of randomized controlled trials. Eur Rev Med Pharmacol Sci 2023; 27(10): 4656–4669. DOI: 10.26355/eurrev_202309_33521.
4. ESGE guideline update on endoscopic management of CBD stones. Endoscopy 2024; 56(4): 345–360. DOI: 10.1055/a-2104-5678.
5. Ramser B, Coleoglou Centeno A, Ferre A, Thomas S, Brooke M, Pieracci F, Morton A. Laparoscopic common bile duct exploration is an effective, safe, and less-costly method of treating choledocholithiasis. Surg Endosc 2024; 38(10): 6076–6082. DOI: 10.1007/s00464-024-10876-2.
6. Anwar M, Abdelmoneim SA, Hamida M, Samir M, Deeba MA, Hassan M, Hany M, Torensma B, Hefzy M. The efficacy of one-stage laparoscopic versus two-stage endo-laparoscopic management of cholecystocholedocholithiasis. BMC Surg 2025; 25(1): 325. DOI: 10.1186/s12893-025-01325-7.
7. Liu F, Ye L, Wang Y, Zhao Z, Mutailipu M, Wang X, Zhang Q, Chen B, Cui R. Short-term efficacy of LCBDE+LC versus ERCP/EST+LC in the treatment of cholelithiasis combined with common bile duct stones: A retrospective cohort study. J Laparoendosc Adv Surg Tech A 2025; 35(2): 145–151. DOI: 10.1089/lap.2024.0345.
8. Custódio VHB, Oliveira AG, Gonçalves FA Jr, Carani JPA, Aguiar IB, Cataneo AJM, Spadella CT. Laparoscopic common bile duct exploration versus pre- or intraoperative endoscopic treatment for choledocholithiasis a systematic review and meta-analysis. European Journal of Pharmaceutical and Medical Research 2023; 10(6): 87–101. DOI: 10.32648/ejpmr.2023.10687.
9. Fang H, Chen W, Wu Z, Ding G. Comparative analysis of minimally invasive approaches for gallbladder and common bile duct stones: Combined endoscopic techniques vs. ERCP with laparoscopic cholecystectomy. Front Surg 2025; 12: 1543205. DOI: 10.3389/fsurg.2025.1543205.
10. Williams E, Beckingham I, El Sayed G, Gurusamy K, Sturgess R, Webster G, Young T. Updated guideline on the management of common bile duct stones (CBDS). Gut 2017; 66(5): 765–782. DOI: 10.1136/gutjnl-2016-312317.
11. Kirkegaard-Klitbo A, Shabanzadeh DM, Olsen MH, Lindschou J, Gluud C, Sørensen LT. One-step laparoscopic cholecystectomy with common bile duct exploration and stone extraction versus two-step endoscopic retrograde cholangiography with stone extraction plus laparoscopic cholecystectomy for patients with common bile duct stones: A randomised feasibility and pilot clinical trial-the preGallStep trial. Pilot Feasibility Stud 2023; 9(1): 21. DOI: 10.1186/s40814-023-01251-z.
12. Garza RA, Rodriguez HA, Guajardo Nieto DA, Treviño Figueroa AM, González Urquijo M, Rendón Macías ME, Alam Gidi AG, Muñiz JJ, Shade MR. Comparison of intraoperative ERCP vs laparoscopic common bile duct exploration for CBD stones in an under-resourced setting. Indian J Surg 2023; 86: 938–943. DOI: 10.1007/s12262-023-03997-5.
13. Varone A, Mendoza A, Gelbard R, Tracy B, Poulose B. Suspected common bile duct stones: Which test is best? Surg Endosc 2025; 39: 6525–6529. DOI: 10.1007/s00464-025-12054-z.