Lietuvos chirurgija ISSN 1392–0995 eISSN 1648–9942
2026, vol. 25(2), pp. 161–169 DOI: https://doi.org/10.15388/LietChirur.2026.25(2).6
Hemorrhoidectomy with LigaSure – an Experience
Mohammad Alfehaid
Qassim University, College of Medicine, Department of Surgery, Saudi Arabia
E-mail: m.alfehaid@qu.edu.sa
https://ror.org/01wsfe280
Abstract. Background. Hemorrhoidectomy using the LigaSure system (LS) is a recent addition to the surgical armamentarium. Aim. To prospectively evaluate the outcomes of LigaSure hemorrhoidectomy in terms of blood loss, postoperative pain, duration of hospitalization, post-operative complications, and patients’ satisfaction. Methods. The records of all the cases who underwent LigaSure hemorrhoidectomy for internal hemorrhoids from June 2019 to May 2025 were analyzed. Demographics, comorbidities, type of anesthesia, procedure time, the volume of blood lost, postoperative pain, duration of hospitalization, post-operative complications, and the feedback expressed by the patients. Results. Out of 140 patients, there were 108 males and 32 females, with a mean age of 39.3 years. 88 (62.9%) cases were managed for Goligher’s grade III, and 52 (37.1%) had grade IV internal hemorrhoids. The mean procedure time was 14.3±3.9 min, respectively. The mean volume of blood lost in the procedure was 13.7 ml. The pain VAS score ranged from 3 to 7 (mean 4.83±0.93) and gradually decreased over 7 postoperative days. The mean duration to return to normal routines of life was 13.8±2.7 days, and 76% of patients were either highly satisfied or satisfied. Conclusion. Haemorrhoidectomy using LigaSure is a safe and effective method for the management of grade III and IV hemorrhoids.
Keywords: hemorrhoids, LigaSure haemorrhoidectomy, LigaSure system, visual analog scale.
Received: 2026-01-21. Accepted: 2026-02-15.
Copyright © 2026 Mohammad Alfehaid. Published by Vilnius University Press. This is an Open Access article distributed under the terms of the Creative Commons Attribution Licence, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction
Internal hemorrhoids are anal submucosal cushions located just proximal to the dentate line and comprised of loose connective tissue, smooth muscle, and blood vessels [1]. They may get expanded, leading to symptoms like bleeding, prolapse, discomfort, thrombosis, mucus discharge, and pruritus. According to Goligher’s classification, there are four grades of internal hemorrhoids according to the degree of protrusion and reducibility [2], as depicted in Figure 1.

Figure 1. Grades of internal hemorrhoids
Hemorrhoidectomy is the most established treatment modality for grades III and IV [3]. It is one of the most frequently performed anorectal surgical operations globally and traditionally has two approaches: Milligan–Morgan’s method (open method) or Ferguson’s method (closed method). These approaches are frequently associated with significant postoperative complications, including pain and prolonged hospital stays, and hence techniques and devices are being suggested from time to time to overcome these adverse issues. The introduction of a new surgical instrument named LigaSureTM (LigH; Medtronic, Dublin, Ireland) is one such innovation in this direction. The LigaSureTM consists of a bipolar electrothermal device that offers an optimized combination of energy and pressure, achieving permanent fusion of vessels up to 7 mm in diameter without any need for dissection or isolation. The average seal cycle is 2‒4 seconds, and the sealed tissue is supposed to withstand three times the normal systolic blood pressure of the patient. The system works on a feedback control system and generates precise thermal energy corresponding to the tissue impedance, thereby allowing the procedure to be conducted in a bloodless field. The thermal impact is confined to a mere 2 mm over the surgical site, and this limited thermal spread has been found to reduce anal spasm and postoperative pain [4]. Furthermore, it has been associated with significantly less surgical time and bleeding in comparison to traditional approaches [5].
It was against this background that this study was undertaken to analyze the outcomes of LigaSure hemorrhoidectomy with respect to blood loss, postoperative pain, duration of hospitalization, post-operative complications, and patients’ satisfaction.
Materials and methods
This is a prospective study conducted at the multiple medical centres under the guidance of Department of Surgery, College of Medicine, Qassim University, Saudi Arabia. The study was undertaken after approval from the departmental ethical committee. The data related to the patients in whom LigaSure hemorrhoidectomy was conducted (by the author) for haemorrhoids from June 2019 to May 2025 was recorded and analyzed. The exclusion criteria included incomplete documentation, history of other anorectal disorders or previous surgical intervention, coagulopathy, and being otherwise medically unfit for anesthesia.
The studied parameters include demographics, comorbidities, type of anesthesia, procedure time, the volume of blood lost during the procedure, duration of hospitalization, post-operative complications including pain on the day of operation and on follow-up, bleeding, difficulty in defecation, and others. Patients were followed up in the surgical outpatient’s department up to 9 months. The time to return to their routine life was noted and feedback was sought to gauge the level of satisfaction and registered as highly satisfied, satisfied, neither satisfied nor dissatisfied, dissatisfied and highly dissatisfied. All the data was recorded in a Microsoft Excel 2020 sheet. The Statistical Product and Service Solutions (SPSS) Statistics 25.0 (IBM Corporation, Armonk, New York) was used to conduct the statistical analyses. Categorical descriptive data were presented as numbers and percentages, and continuous descriptive data were expressed as the mean and standard deviation. Unpaired t-test was used to analyze the results summarized as means, whereas the results summarized as percentages were analyzed by Fisher’s exact test. A p-value of <0.05 was considered statistically significant.
Surgical procedure
The patients were evaluated preoperatively by anesthesia teams and optimized. Colonic pathology was ruled out by colonoscopy in 46 (32.9%) cases where there was any suspicion of a possible colonic pathology including any patient above age of 45 years. Incontinence was ruled out in all patients preoperatively using the Wexner continence scoring system. The various options for management were offered, and the patients opting for LigaSure were enrolled in the study after proper explanation and assurance of maintaining anonymity. Antiplatelets, if any, were discontinued 7 days before the procedure in consultation with the internal medicine department. The bowel was cleansed by rectal enema about a 6 hour before the operation. Antibiotic prophylaxis with 1 g of third-generation cephalosporin IV was administered.
A hemorrhoidectomy was performed with LigaSureTM Small Jaw/Precise (Medtronic, Dublin, Ireland). After positioning the patient in the lithotomy position and applying an anal retractor, a V-shaped incision was marked with a marking pen, and an anodermal wedge was incised with a electrocautery LigaSure was engaged, and en-bloc excision of hemorrhoidal masses was undertaken one by one. A hemostatic sponge was placed for compression of the anal canal, and the operation was completed.
In the postoperative period, the patient was regularly administered paracetamol and pethidine for analgesia until discharge, and on discharge, paracetamol and codeine preparations were advised for use as required (PRN). They were advised Sitz bath and prescribed oral liquid lactulose. The patients and caregivers were taught the Visual Analogue Scale (VAS) and advised to record the maximum level of pain every day until follow-up at one week.
Results
A total of 146 patients underwent LigH for grade III and IV hemorrhoidal disease from June 2019 to May 2025; 6 patients were lost to follow-up after three weeks, and hence, only 140 patients were included in the study. There were 108 (77.1%) males and 32 (22.9%) females, ranging in age from 24 years to 80 years (mean 39.3 years), as shown in Figure 2. Ten patients (8 males and 2 females) were over 60 years old and hence categorized as elderly. 88 (62.9%) cases had Goligher’s grade III, and 52 (37.1%) had grade IV internal hemorrhoids. The co-morbidities included controlled hypertension in 12 (8.6%), type 1 diabetes mellitus in 8 (5.7%), hyperplasia of the prostrate in 8 (5.7%), and bronchial asthma in 6 (4.3%) cases.

Figure 2. Gender and age distribution of patients
The hospital stay was 1 day for 134 (95.7%) cases and 2 days for 6 (4.3%) cases. Two (1.4%) cases required readmission for 1 and 4 days, respectively, due to postoperative complications. The mean hospital stay was 1.1 days. A single haemorrhoid mass was excised in 38 (27.1%), two in 92 (65.7%), and three in 10 (7.2%). The procedure was conducted under spinal anesthesia in 105 (75%), general 34 (24.3%), and local 1 (10.7%). Local anesthesia was used in cases of paraplegia (post-spinal cord injury).
The operative time (after the exclusion of time taken by the anesthesia team) ranged from 8 to 28 min, as shown in Figure 3. Overall mean operation time was 14.3±3.9 min, and mean time for excision of one, two, and three haemorrhoids was 10.6±١.٩٥ min, 14.7±٢.٢٧ min, and 24.6±٤.١٨ min; the difference in operation time with respect to the number of hemorrhoids cushions was significant (p ≤ 0.001).
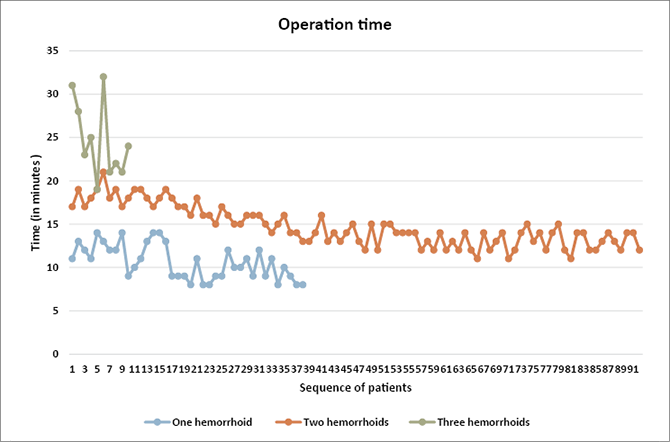
Figure 3. Operation time of LigaSure haemorrhoidectomy
Overall mean blood loss during the operation was 13.7 ml, and the values of mean blood loss were 9.2 ml, 15.1 ml, and 18.4 ml, respectively, after the excision of one, two, and three hemorrhoids, as shown in Table 1. No significant intraoperative complications were witnessed.
Table 1. Blood loss during LigaSure haemorrhoidectomy
|
Blood loss during operation |
|||
|
Number of excised |
Minimum (ml) |
Maximum (ml) |
Mean (ml) |
|
1 |
5 |
14 |
9.2 |
|
2 |
10 |
20 |
15.1 |
|
3 |
15 |
22 |
18.4 |
The pain VAS score within 24 hours of the operation (Day 0) ranged from 3 to 7 (mean 4.83±0.93), and the pain VAS score gradually decreased over 7 postoperative days, as shown in Figure 4.

Figure 4. Postoperative pain as assessed with Visual analogue scale
However, pain reappeared in the second week, with scores of 7 and 9 in two cases that required re-admissions. One 77-year-old male developed faecal impaction and required digital evacuation under sedation; in the second, secondary hemorrhage occurred in a 32-year-old male patient on 9th postoperative day and was managed conservatively with antibiotics, analgesia, and closed observation. The other complications included urinary retention requiring urinary catheterization in 4 (2.6%) cases from the elderly age group, temporary incontinence to gas and fluids lasting up to the maximum of 2 weeks in 10 (7.1%) cases, and minor bleeding (a few drops) after defecation lasting up to the maximum of 3 weeks in 18 (12.9%) cases across all age groups and both genders.
The time taken to return to daily activities ranged from 8 to 20 days (mean 13.8±2.7 days). The two patients requiring readmission were last to return to routine life (at 20 days). Neither the gender of the patients nor the grade of their hemorrhoids had any statistically significant impact on the parameters. At 9 months of follow-up, 12 (8.6%) patients had evidence of grade II internal hemorrhoids, and 2 (1.4%) patients had features of a chronic anal fissure. They were managed conservatively. The levels of satisfaction of the patients were ‒ highly satisfied (n = 38; 27%), satisfied (n = 82; 59%), neither satisfied nor dissatisfied (n = 14; 10%) and dissatisfied (n = 6; 4%) as depicted in Figure 5.

Figure 5. Level of satisfaction after Ligasure haemorrhoidectomy
Discussion
Excisional haemorrhoidectomy is the mainstay operation for Goligher’s grade III and IV haemorrhoids, and to minimize potential postoperative difficulties, many different approaches and tools have been devised [3, 6]. LigaSure hemorrhoidectomy is one such recent addition to surgical armamentarium, and this modality has improved further in recent years with the introduction of more practice-effective and ergonomic forceps (LigaSure Precise) with shorter and slimmer jaws to facilitate hemorrhoids dissection off the internal anal sphincter, thereby limiting the extent of thermal injury to only a millimetre [7].
The mean operation in this series was 14.3±3.9 min, and the operation time got prolonged significantly with the number of hemorrhoids removed. The operation time concurs with the timing mentioned in the literature. Rahman et al. [8] achieved a mean operation time of 15.25 min, and the operation time for single cushions was 9.2±1.25 min. In a series by Elsayed [9], the mean procedure time was 12.5±3 min. Aljabery and Jaber [10] achieved a mean operation time of 12.2±3 min. In a series by Khanna et al. [11], the average operating time was 12.5±3 min. However, the mean operation time for LigaSure hemorrhoidectomy in a randomized controlled trial conducted by Gentile et al. [12] was 22.3 min.
LigaSure hemorrhoidectomy creates wounds in anoderm, which is very sensitive and hence leads to pain, though that is less than conventional approaches [13]. The pain VAS score in this series was 4.83±0.93 within 24 hours of the operation (Day 0), and the score gradually decreased over the week. In a series by Gentile et al. [12], the maximum VAS score on the day of surgery was 3.7 and gradually dropped to 1.6 on the fourth postoperative day. In the series by Chen et al. [14], the mean pain score on the day of operation was 3. In the series by Elsayed [9], VAS on the day of operation was 4.1±0.8 and reached 1.2±0.2 by seven days. Similarly, the hospitalization days were very similar to those in other series. In this series, the mean hospital stay was 1.1 days, and in the series by Elsayed [9], it was 1.4. Milito et al. [13] reported an operation time of 9.2 min and a mean hospital stay of 1.8 days with the use of the Ligasure. Milito et al. [13] have suggested an intensive aftercare protocol after Ligasure with the use of sphincter relaxants like glycerin trinitrate ointment in addition to the usual classic painkillers. Furthermore, the use of topical metronidazole is supported, supposing that infection at the site of anal wounds has a role in postoperative pain [15].
A 77-year-old male required readmission on 7th postoperative day for faecal impaction. Chen et al. [14] assessed the association between age and outcomes in patients undergoing LigaSure hemorrhoidectomy by comparing the baseline characteristics and surgical outcomes in 1 075 cases under 65 years of age with 163 cases with an age greater than 65 years. They found that the LigaSure hemorrhoidectomy for elderly patients is safe and effective without any statistically significant difference in perioperative outcomes or complications when compared with younger patients. The whole course of the procedure was tolerated in the prone jackknife position without anesthesia-associated complications [14]. Selvaggio et al. [16], after analysis of the data of 152 elderly patients with grade III or IV symptomatic hemorrhoids who underwent LigaSure hemorrhoidectomy, concluded that the approach is safe, simple, reproducible, and fast even for geriatric patients, with a low rate of early and late postoperative complications.
Secondary hemorrhage was the cause of readmission in a 32-year-old male. The patient was readmitted on the 9th postoperative day and managed conservatively. There have been reports of postoperative bleeding following LigaSure hemorrhoidectomy ranging from 0.9% to 10% in various studies [14]. Chen et al. [14] demonstrated that older patients did not have a higher risk of postoperative hemorrhage. However, although there was no statistical significance, older individuals tended to have less delayed bleeding. Most elderly patients are retired and can rest longer following surgery, which may explain the cause. The reason for delayed bleeding may be local infection of the ligated pedicle, suture erosion, or oozing from edges of the unhealed operation site. In our series, LigaSure hemorrhoidectomy was performed in a sutureless fashion in all the patients, though some series [14] mention the application of some stitches on the LigaSure welting line to prevent postoperative bleeding.
Altomare [7] has discussed the issue of intra- and postoperative hemorrhage in LigaSure haemorrhoidectomy at length and made various recommendations. Persistent intraoperative hemorrhage can be controlled with repeated application of the LigaSure device, coagulation with classic diathermy, or the application of re-absorbable sutures. For postoperative hemorrhage, Altomare [7] suggests that the management should not be different from post-haemorrhoidectomy hemorrhage after other surgical approaches and that adoption of a conservative treatment is preferred with the use of intravenous procoagulants and local hemostatic products. However, a surgical revision is a must if haemoglobin level drops to under 8 g/l, and the patient should not be discharged until bleeding is stopped and first defecation occurs. Cheng et al. [17], in a study, tried to identify the risk factors for delayed hemorrhage after LigaSure haemorrhoidectomy and found that male sex was an independent risk factor. They found that the risk is higher in patients undergoing the procedure in a surgeon’s earlier cases and decreases to a rate like that for the traditional hemorrhoidectomy once the surgeon attains experience in the procedure and the postoperative care.
In this series, patients were operated upon on either general or spinal anesthesia, and in the only case of paraplegia post-spinal cord injury, the procedure was undertaken in the operating room under local anesthesia. In a recent study, Feo et al. [18] evaluated the safety and efficacy of local anesthesia in the outpatient clinic vs. spinal anesthesia in the operating room for LigaSure hemorrhoidectomy, enrolling 62 patients, of whom 30 were operated on in the outpatient clinic under local anesthesia with ropivacaine and the other 32 cases were operated on in the operating room under spinal anesthesia with hyperbaric bupivacaine. No statistically significant differences were observed in postoperative pain, perioperative complications, reoperation rate, recurrences, or the degree of patients’ satisfaction, thereby concluding that hemorrhoidectomy with LigaSure can be safely and effectively performed in selected patients under local anesthesia in the outpatient clinic.
Over the last two decades, LigaSure hemorrhoidectomy has been compared with traditional and other newer modalities in various trials and studies. This modality has been proven to be safe and effective without significant differences in short-term operative outcomes or complication rates across all age groups. Sakr [4], Baig et al. [5], Elsayed [9], Aljabery et al. [10], and Gentile et al. [12] compared LigaSure hemorrhoidectomy with Milligan‒Morgan hemorrhoidectomy, whereas Khanna et al. [11] and Xu et al. [19] compared conventional Ferguson’s hemorrhoidectomy.
Chen et al. [20] conducted a meta-analysis of randomized control trials to compare Ligasure with stapled hemorrhoidectomy and found that operation time and recurrence rates were lower in the former, though no statistically significant differences were observed in other variables including postoperative pain, postoperative hemorrhage, urinary retention, difficulty in defecation, anal fissure, anal stenosis, incontinence, return to normal activities, and hospital stay. Yang et al. [21] also concluded that SH and LH are almost equally valuable techniques in modern haemorrhoid management, though LigaSure might offer somewhat favourable immediate postoperative results and technical advantages.
Conclusions
Hemorrhoidectomy using LigaSure is a safe and effective procedure across all age groups and genders. There is minimal tissue trauma, and there is no need to use sutures or staples.
Disclosures
The author has not received any funds, sponsorships, or any other financial or non-financial benefits from any governmental or non-governmental agencies or pharmaceutical companies, and this study has been conducted purely for academic pursuits.
Conflict of interest
No conflict of interest.
Acknowledgements
The author expresses gratitude to the patients for allowing the usage of their data for academic purposes; however, there is no consent for any use of images related to the operation and hence, no peroperative images have been added to the article.
Data Availability Statement
This data related to this article may be provided upon appropriate request.
References
1. Durgun C, Yigit E. Laser hemorrhoidoplasty versus ligasure hemorrhoidectomy: A comparative analysis. Cureus 2023; 15(8): e43119. DOI: 10.7759/cureus.43119.
2. Madoff RD, Fleshman JW. American Gastroenterological Association technical review on the diagnosis and treatment of hemorrhoids. Gastroenterology 2004; 126(5): 1463‒1473.
3. Lohsiriwat V. Treatment of hemorrhoids: A colo-proctologist’s view. World J Gastroenterol 2015; 21(31): 9245‒9252.
4. Sakr MF. LigaSure versus Milligan‒Morgan hemorrhoidectomy: A prospective randomized clinical trial. Tech Coloproctol 2010, 14: 13‒17.
5. Baig AA, Mehmood MS, Khalid R, Ghufran S, Chaudhry SM, Mehbub H. Comparative study between Milligan‒Morgan versus Ligasure haemorrhoidectomy. Pakistan J Med Health Sci 2022; 16: 235.
6. Yeo D, Tan KY. Hemorrhoidectomy ‒ making sense of the surgical options. World J Gastroenterol 2014; 20: 16976‒16983.
7. Altomare DF. Tips and tricks: Hemorrhoidectomy with LigaSure. Tech Coloproctol 2009; 13: 321‒322.
8. Rahman FU, Amin A, Nisar S, Musarat H. Outcome of hemorrhoidectomy with the LigaSure in comparison with the traditional open method. JGMDS 2017; 4(1): 4‒7.
9. Elsayed MEN. A comparison between the outcome of LigaSure hemorrhoidectomy versus conventional Milligan‒Morgan’s technique. AIMJ 2022; 3(1): 52‒56.
10. Aljabery RMS, Jaber AAS. Comparison of hemorrhoidectomy by Ligasure with conventional Milligan‒Morgan’s hemorrhoidectomy. Medico-legal update 2020; 20(1): 1324‒1328.
11. Khanna R, Khanna S, Bhadani S, Singh S, Khanna AK. Comparison of ligasure hemorrhoidectomy with conventional Ferguson’s hemorrhoidectomy. Indian J Surg 2010; 72(4): 294‒297.
12. Gentile M, De Rosa M, Carbone G, Pilone V, Mosella F, Forestieri P. LigaSure haemorrhoidectomy versus conventional diathermy for IV-degree haemorrhoids: Is it the treatment of choice? A randomized, clinical trial. ISRN Gastroenterol 2011; 467258: 6.
13. Milito G, Gargiani M, Cortese F. Randomised trial comparing LigaSure hemorrhoidectomy with the diathermy dissection operation. Tech Coloproctol 2002; 6(3): 171‒175.
14. Chen CW, Lu TJ, Hsiao KJ. Surgical outcomes of LigaSure hemorrhoidectomy in the elderly population: A retrospective cohort study. BMC Gastroenterol 2021; 21: 413.
15. Ala S, Saeedi M, Eshghi F, Mirzabeygi P. Topical metronidazole can reduce pain after surgery and pain on defecation in postoperative hemorrhoidectomy. Dis Colon Rectum 2008; 51: 235–238.
16. Selvaggio I, Cadeddu F, Muzi MG, Andreoli F, Amabile D, Milito G. Milligan‒Morgan haemorrhoidectomy with LigaSure in geriatric patients. BMC Geriatrics 2009; 9(Suppl 1): A99.
17. Cheng KC, Song LC, Wu KL, Chen HH, Lee KC. Risk factors of delayed hemorrhage after LigaSure hemorrhoidectomy. BMC Surg 2022; 22(1): 361.
18. Feo CF, Ninniri C, Tanda C, Deiana G, Porcu A. Open hemorrhoidectomy with Ligasure™ under local or spinal anesthesia: A comparative study. Am Surg 2023; 89(4): 671‒675.
19. Xu L, Chen H, Lin G, Ge Q. Ligasure versus Ferguson hemorrhoidectomy in the treatment of hemorrhoids: A meta-analysis of randomized control trials. Surg Laparosc Endosc Percutan Tech 2015; 25(2): 106‒110.
20. Chen HL, Woo XB, Cui J, Chen CQ, Peng JS. Ligasure versus stapled hemorrhoidectomy in the treatment of hemorrhoids: A meta-analysis of randomized control trials. Surg Laparosc Endosc Percutan Tech 2014; 24(4): 285‒289.
21. Yang J, Cui PJ, Han HZ, Tong DN. Meta-analysis of stapled hemorrhoidopexy vs. LigaSure hemorrhoidectomy. World J Gastroenterol 2013; 19(29): 4799‒4807.