Lietuvos chirurgija ISSN 1392–0995 eISSN 1648–9942
2026, vol. 25(2), pp. 107–123 DOI: https://doi.org/10.15388/LietChirur.2026.25(2).1
Prophylaxis and Management of Deep Vein Thrombosis in Surgical Patients ‒ a Narrative Review
Muhammad Munir Memon
Qassim University, College of Medicine,
Department of Surgery, Kingdom of Saudi Arabia
E-mail: m.ghafar@qu.edu.sa
https://orcid.org/0000-0003-2501-3126
Zaheera Saadia
Qassim University, College of Medicine,
Department of Gynecology, Kingdom of Saudi Arabia
E-mail: saadia@qu.edu.sa
Manar Mohammed Al Qapa
Qassim University, College of Medicine,
Kingdom of Saudi Arabia
E-mail: 391202261@qu.edu.sa
Hessah Abdulrahman Alkhudair
Qassim University, College of Medicine,
Kingdom of Saudi Arabia
E-mail: 431201309@qu.edu.sa
Modhi Saleh Alfraidi
Qassim University, College of Medicine,
Kingdom of Saudi Arabia
E-mail: 382225357@qu.edu.sa
Nouf Dalli Alenezi
Qassim University, College of Medicine,
Kingdom of Saudi Arabia
E-mail: 431201445@qu.edu.sa
Nouf Nawaf Alharbi
Qassim University, College of Medicine,
Kingdom of Saudi Arabia
E-mail: 411214704@qu.edu.sa
Maryam Mousa Alharbi
Qassim University, College of Medicine,
Kingdom of Saudi Arabia
E-mail: 431201413@qu.edu.sa
Lama Abdullah Alharbi
Qassim University, College of Medicine,
Kingdom of Saudi Arabia
E-mail: 391202573@qu.edu.sa
Wateen Mohammad Alharbi
Qassim University, College of Medicine,
Kingdom of Saudi Arabia
E-mail: 431201834@qu.edu.sa
Wafaa Abdulaziz Alhudithi
Qassim University, College of Medicine,
Kingdom of Saudi Arabia
E-mail: 391202305@qu.edu.sa
Abstract. Venous thromboembolism (VTE), encompassing deep vein thrombosis (DVT) and pulmonary embolism (PE), persists as a leading cause of preventable perioperative morbidity and mortality. Surgical patients are at variable and often substantial risk due to the synergistic effects of immobility, tissue injury, inflammation, and underlying comorbidities. Contemporary best practice is founded upon individualized risk assessment, the judicious application of pharmacological prophylaxis, primarily low-molecular-weight heparin (LMWH), and mechanical measures, coupled with a clear strategy for managing patients on chronic anticoagulation. For established VTE, direct oral anticoagulants (DOACs) have streamlined long-term management, though LMWH remains paramount in specific populations such as patients with cancer. This narrative review synthesizes current evidence and guidelines for the prevention and treatment of perioperative VTE, incorporating recent literature to inform clinical practice. Individualized prophylaxis guided by validated risk models and adherence to evidence-based protocols remains pivotal in reducing perioperative VTE morbidity and mortality.
Keywords: deep vein thrombosis (DVT), venous thromboembolism (VTE), surgical prophylaxis, anticoagulant therapy, low-molecular-weight heparin (LMWH), direct oral anticoagulants (DOACs), mechanical thromboprophylaxis, perioperative management, postoperative complications, risk assessment models, thromboprophylaxis guidelines, pulmonary embolism prevention.
Received: 2026-01-02. Accepted: 2026-02-01.
Copyright © 2026 Muhammad Munir Memon, Zaheera Saadia, Manar Mohammed Al Qapa, Hessah Abdulrahman Alkhudair, Modhi Saleh Alfraidi, Nouf Dalli Alenezi, Nouf Nawaf Alharbi, Maryam Mousa Alharbi, Lama Abdullah Alharbi, Wateen Mohammad Alharbi, Wafaa Abdulaziz Alhudithi. Published by Vilnius University Press. This is an Open Access article distributed under the terms of the Creative Commons Attribution Licence, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction
Venous thromboembolism remains a formidable complication in surgical care, transcending procedural boundaries and specialties. Postoperative DVT and PE can prolong hospitalization, precipitate readmissions, lead to chronic debilitating conditions like post-thrombotic syndrome, and result in fatal outcomes [1]. Consequently, the prevention and prompt management of VTE are critical pillars of surgical quality and patient safety (Figure 1). The central challenge lies in meticulously balancing the reduction of thrombotic risk against the inherent potential for bleeding, a nuanced decision-making process in a highly heterogeneous patient population [2].

Figure 1. Deep vein thrombosis of the right leg ‒ a clinical photo showing typical signs (swelling, redness) of DVT in a leg. CC BY-SA 3.0 (Wikimedia Commons).
{kind=link}
Epidemiology and impact in surgical patients
The incidence of clinically significant postoperative VTE varies considerably, influenced by the type of procedure, the presence of underlying disease (notably malignancy), and specific patient factors [3]. Major abdominal and pelvic operations, oncologic surgery, major orthopedic procedures (e.g., hip and knee arthroplasty), and trauma are consistently identified as high-risk contexts [4]. It is crucial to recognize that even asymptomatic DVT, often detected only through routine screening, is associated with subsequent morbidity and increased healthcare costs [5]. Furthermore, a significant proportion of surgical VTEs manifest after hospital discharge, underscoring the critical importance of adequate post-discharge planning, including the consideration of extended-duration pharmacological prophylaxis [6].
Pathophysiology ‒ Virchow’s triad and surgery
The pathogenesis of perioperative VTE is elegantly explained by Virchow’s triad, which surgery potently activates (Figures 2a and 2b). The triad comprises: (1) endothelial injury from direct surgical trauma and dissection; (2) venous stasis due to intraoperative immobilization, anesthesia, and reduced postoperative mobility; and (3) hypercoagulability driven by the acute phase response, inflammation, and perioperative shifts in the coagulation cascade [7]. Additional contributory factors include dehydration, venous compression, the presence of central venous catheters, and the profound prothrombotic state associated with active malignancy [8].

Figure 2a. Virchow’s triad of factors that lead to thrombosis
Figure 2b. Pathophysiology of deep vein thrombosis showing thrombus formation and propagation.
Source: EM Daily (Creative Commons Educational Material). License: CC BY 4.0.
Virchow’s triad describes the three broad categories of factors that are thought to contribute to thrombosis: hypercoagulability, hemodynamic changes (stasis, turbulence), and endothelial injury/dysfunction. This file is licensed under the Creative Commons Attribution-ShareAlike 3.0 Unported license.
Anatomy and investigations
To understand more about the subject, there is a sketch of anatomy of the veins of the lower limb (Figures 3a and 3b).

Figure 3a. Detailed anterior and posterior venous anatomy of the lower limb.
Source: U.S. National Cancer Institute (NCI). Public domain.
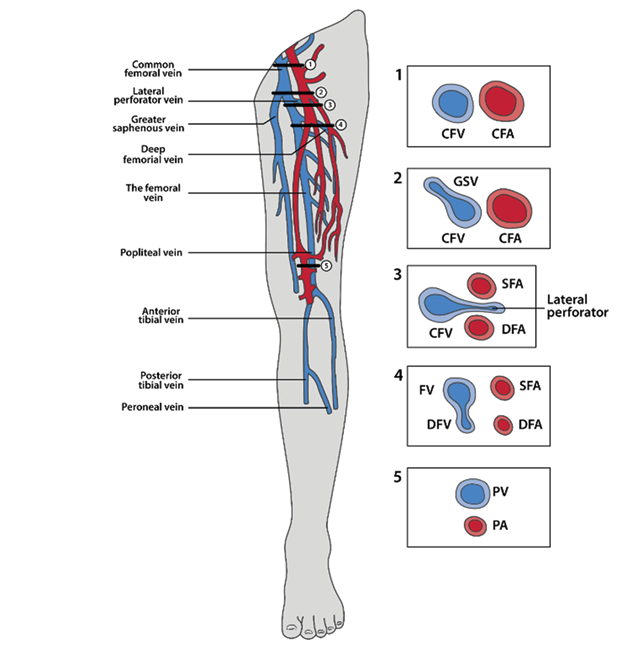
Figure 3b. Lower extremity venous anatomy relevant to point-of-care ultrasound (POCUS) evaluation for DVT. Adapted from UBC Emergency Medicine. License: CC BY 4.0.
Best modality of investigation is Doppler ultrasound in this regard (Figures 4a and 4b).
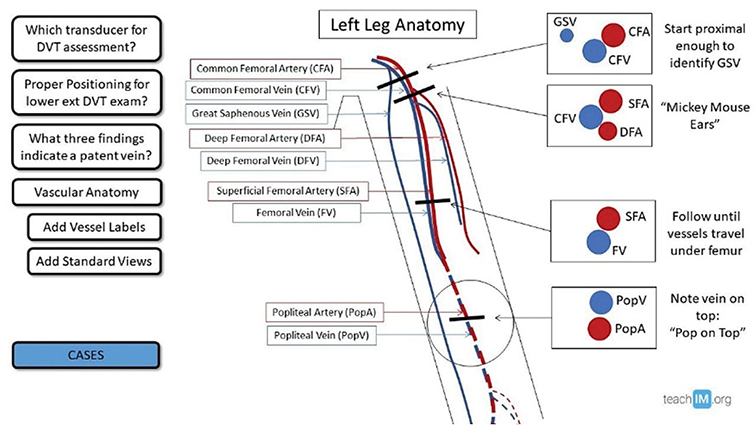
Figure 4a. Compression ultrasound technique for evaluati on of deep vein thrombosis.
Source: TeachIM. License: CC BY 4.0.

Figure 4b. Doppler ultrasonography of the right leg of a 65-year-old man with a swollen right leg. It shows deep vein thrombosis in the sub scrotal vein. There is absence of blood flow as well as hyper echogenicity in the thrombosed vessel, as compared to the deep femoral vein and the femoral artery. Ultrasound demonstrating non-compressibility of the femoral vein consistent with acute deep vein thrombosis. Source: U.S. National Library of Medicine contributors. Public domain (CC0).
Risk assessment
Personalized prophylaxis commences with a formal, structured risk assessment. Several validated clinical risk stratification tools are widely employed.
The Caprini score is extensively validated in general surgical populations, stratifying patients into risk categories from very low to highest risk, which directly informs the intensity and duration of prophylactic measures [9].
It helps clinicians decide who needs prophylaxis (e.g., compression stockings, low molecular weight heparin [LMWH], etc.) and how aggressive that prophylaxis should be.
Its purpose to stratify patients into low, moderate, high, or very high risk of VTE based on individual and surgical factors.
Table 1. Caprini risk assessment model for DVT prophylaxis
|
Risk factor |
Points |
|---|---|
|
Age 41–60 years |
1 |
|
Minor surgery |
1 |
|
BMI > 25 kg/m² |
1 |
|
Swollen legs |
1 |
|
Varicose veins |
1 |
|
Pregnancy or postpartum |
1 |
|
Oral contraceptives or hormone replacement therapy (HRT) |
1 |
|
Sepsis (<1 month) |
1 |
|
Age 61–74 years |
2 |
|
Arthroscopic or laparoscopic surgery >45 minutes |
2 |
|
Malignancy (current or previous) |
2 |
|
Major open surgery >45 minutes |
2 |
|
Central venous access |
2 |
|
Age ≥75 years |
3 |
|
Prior VTE (DVT or PE) |
3 |
|
Family history of VTE |
3 |
|
Known thrombophilia (e.g., Factor V Leiden, prothrombin G20210A, lupus anticoagulant, anticardiolipin antibody) |
3 |
|
Stroke (<1 month) |
5 |
|
Multiple trauma (<1 month) |
5 |
|
Acute spinal cord injury (<1 month) |
5 |
|
Elective lower-extremity arthroplasty |
5 |
|
Hip, pelvic, or leg fracture |
5 |
Table 2. Risk stratification and recommended prophylaxis
|
Total points |
Risk level |
Approximate DVT risk |
Recommended prophylaxis |
|---|---|---|---|
|
0 |
Very low |
<0.5% |
Early ambulation only |
|
1–2 |
Low |
~1.5% |
Mechanical prophylaxis (e.g., graduated compression stockings or intermittent pneumatic compression) |
|
3–4 |
Moderate |
~3% |
LMWH or low-dose UFH or mechanical methods |
|
≥5 |
High/very high |
6–10% + |
LMWH + mechanical methods (if not contraindicated) |
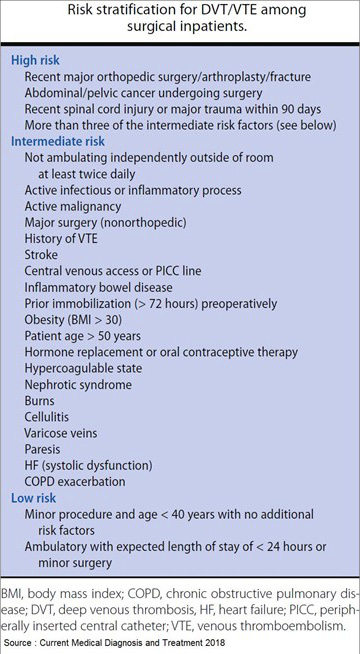
Figure 5. Risk stratification for DVT/VTE among surgical patients
This model serves as a clinical guide. Always consider individual patient factors, comorbidities, and institutional protocols when deciding on DVT prophylaxis.
Examples of prophylactic measures
• Mechanical: graduated compression stockings (GCS), intermittent pneumatic compression (IPC).
• Pharmacologic:
▪ Low molecular weight heparin (e.g., enoxaparin 40 mg SC daily).
▪ Unfractionated heparin (5,000 U SC every 8–12 h).
▪ Fondaparinux 2.5 mg SC daily (selected patients).
Duration depends on risk and type of surgery (often 7–10 days; extended to 4 weeks after major cancer or orthopedic surgery).
Why the Caprini score matters
• It is endorsed by the American College of Chest Physicians (ACCP) and American Society of Hematology (ASH) guidelines.
• It is especially useful in general, vascular, and plastic surgery.
• It personalizes prophylaxis, avoiding both under- and over-treatment.
Summary: the Caprini Score is a point-based tool to evaluate venous thromboembolism (VTE) risk in surgical patients and guide DVT prophylaxis choice and intensity.
• Procedure-based risk stratification acknowledges that certain operations, such as major joint arthroplasty or pelvic cancer resections, confer a high baseline VTE risk even in patients without additional risk factors [10].
• Bleeding risk assessment is equally critical. Active bleeding, inherent coagulopathies, or procedures with a high risk of hemorrhage may contraindicate pharmacologic prophylaxis initially, necessitating a reliance on mechanical modalities [11].
A practical clinical approach involves:
1. Performing a preoperative VTE risk assessment using a validated tool like the Caprini score.
2. Systematically documenting the patient’s bleeding risk.
3. Formulating a definitive prophylaxis plan (pharmacological, mechanical, or combined) and determining its intended duration (Table 3).
Table 3. Risk factors for DVT in surgical patients
|
Category |
Specific factors |
|
Patient-related |
Age >60 years, obesity, malignancy, prior DVT/PE, thrombophilia, immobility, estrogen therapy. |
|
Procedure-related |
Major orthopedic, pelvic, or abdominal surgery; prolonged anesthesia; laparoscopic >2 hours. |
|
Postoperative factors |
Dehydration, infection, prolonged immobilization. |
Pharmacological prophylaxis
Agents and general principles
• Low-molecular-weight heparin (LMWH) (e.g., enoxaparin, dalteparin) is the cornerstone of pharmacological prophylaxis due to its predictable pharmacokinetics, once-daily dosing, and reduced need for monitoring compared to unfractionated heparin (UFH) [12].
• Unfractionated heparin (UFH) (subcutaneous, typically 5000 units two or three times daily) remains a valuable option in scenarios where rapid reversibility is desired or in patients with severe renal impairment (CrCl <30 mL/min), as it is not renally cleared [13].
• Fondaparinux, a synthetic factor Xa inhibitor, is highly effective but has a long half-life and lacks a specific reversal agent, warranting caution in patients with renal insufficiency [14].
• Direct oral anticoagulants (DOACs) such as apixaban and rivaroxaban are well-established for VTE prophylaxis following elective hip and knee arthroplasty and are increasingly used for the treatment of established VTE [15]. However, their role for routine prophylaxis in broader general surgical populations is less defined and must be individualized, considering bleeding risk and the timing of surgery [16].
• Aspirin has a recognized role in some orthopedic surgery VTE prevention pathways but is generally not considered an adequate substitute for anticoagulants in moderate-to-high-risk general surgery patients [17].
Timing, dose, and duration
• Timing. The initiation of pharmacologic prophylaxis is a key decision. Preoperative dosing (e.g., 12 hours before surgery) can reduce the risk of intraoperative DVT but may increase bleeding risk. Consequently, many institutions adopt a postoperative initiation strategy (e.g., 6‒12 hours after surgery) for procedures with a high bleeding risk [18].
• Dose. Dosing should be adjusted for patient weight and renal function. Obese patients (BMI >40 or weight >120 kg) may require higher doses of LMWH for effective prophylaxis [19].
• Duration. For most general surgery patients, prophylaxis continues until sufficient ambulation is achieved.
• Extended prophylaxis (up to 4 weeks post-discharge) is strongly recommended after major abdominal or pelvic surgery for cancer and in other high-risk patients (e.g., those with a prior VTE history or persistent immobility) [20]. In orthopedic arthroplasty, extended prophylaxis for up to 35 days is standard [21] (Figures 6a and 6b).

Figure 6a. Schematic overview of the coagulation cascade and the mechanisms of action of the various anticoagulants. TF: tissue factor; VKA: vitamin K antagonist. Illustration by Barry van Varik (Pulse Medical Art). License: CC BY-NC 4.0.

Figure 6b. Coagulation cascade and major classes of anticoagulants. Simplified coagulation cascade showing major classes of anticoagulants and their sites of action. Source: Wikimedia Commons (SteveKong3). License: CC BY-SA 4.0.
Mechanical prophylaxis
• Intermittent pneumatic compression (IPC) devices and graduated compression stockings (GCS) reduce venous stasis and enhance fibrinolysis, thereby lowering DVT risk [22].
• These modalities are indispensable for patients with an absolute contraindication to anticoagulation and serve as valuable adjuncts to pharmacologic prophylaxis in high-risk scenarios.
• The efficacy of IPC is contingent upon consistent wear time; poor adherence significantly diminishes its protective benefit [23] (Table 4).
Table 4. Mechanical methods of DVT prophylaxis
|
Method |
Mechanism of action |
Indications |
Advantages |
Limitations |
|---|---|---|---|---|
|
GCS |
Improves venous return |
Mild-moderate risk, or contraindication to anticoagulants |
Simple, |
Poor compliance |
|
IPC |
Cyclic compression → venous emptying |
High-risk or when anticoagulants contraindicated |
Non-invasive, |
Requires equipment, monitoring |
Combination strategies
For the highest-risk surgical patients, a combination of pharmacological and mechanical prophylaxis provides superior protection compared to either modality alone [24]. Institutional protocols frequently mandate such combined approaches for patients undergoing major cancer surgery or those with multiple VTE risk factors.
Special populations and special surgical scenarios
• Orthopedic surgery. Given the exceptionally high baseline risk, well-defined regimens using DOACs or LMWH for a extended period (up to 35 days) are standard of care [21].
• Oncologic surgery. The prothrombotic nature of malignancy necessitates aggressive prophylaxis. Extended prophylaxis with LMWH for 4 weeks postoperatively is recommended following major abdominal or pelvic cancer surgery, demonstrating a significant reduction in VTE events without a major increase in bleeding [25].
• Bariatric surgery. High VTE risk coupled with altered pharmacokinetics necessitates tailored strategies, including early ambulation, weight-based LMWH dosing, and mechanical prophylaxis [26].
• Trauma and spinal surgery. The balance between high thrombotic risk and bleeding risk is delicate. Mechanical prophylaxis is initiated immediately, with pharmacologic agents introduced as soon as it is deemed safe, often requiring multidisciplinary input [27].
• Renal impairment. Dose adjustments for LMWH and fondaparinux are essential; UFH is often preferred in severe renal failure.
• Pregnancy. LMWH is the agent of choice for prophylaxis and treatment; DOACs are contraindicated due to teratogenic potential [28] (Tables 5 and 6).
Table 5. Recommended thromboprophylaxis according to risk level
|
Risk category |
Example procedures |
Recommended |
Duration |
|---|---|---|---|
|
Low |
Minor surgery, early ambulation |
Early ambulation |
Until discharge |
|
Moderate |
General surgery >45 min, laparoscopic >60 min |
LMWH or UFH or IPC |
7–10 days |
|
High |
Major orthopedic, pelvic, or oncologic surgery |
LMWH + mechanical |
10–14 days |
|
Very high |
Hip/knee replacement, major trauma |
LMWH/DOACs ± IPC |
4–6 weeks |
Table 6. Pharmacologic agents used for DVT prophylaxis
|
Drug/class |
Dosage |
Timing |
Major contraindications |
Notes |
|---|---|---|---|---|
|
UFH |
5,000 U SC q8–12 h |
2 h pre-op/ post-op |
Active bleeding, thrombocytopenia |
Short half-life |
|
LMWH |
40 mg SC daily |
12 h pre-op/ post-op |
Renal impairment |
Adjust for CrCl <30 mL/min |
|
DOACs (Apixaban, Rivaroxaban) |
Apixaban 2.5 mg BID/ Rivaroxaban 10 mg OD |
6–12 h post-op |
Renal/hepatic failure |
Mainly orthopedic use |
Perioperative management of patients on chronic anticoagulant and antiplatelet therapy
This management is guided by the indication for anticoagulation (e.g., atrial fibrillation, mechanical heart valve, recent VTE), the patient’s thrombotic risk if anticoagulation is interrupted, and the bleeding risk of the planned procedure.
• DOACs. Typically withheld 24‒48 hours before surgery (longer with renal impairment). Bridging anticoagulation is generally not required for atrial fibrillation but may be considered for very high-risk conditions like mechanical mitral valves [29].
• Vitamin K antagonists (e.g., warfarin). Discontinued 3‒5 days preoperatively. Bridging therapy with therapeutic-dose UFH or LMWH is used selectively based on thrombotic risk stratification [30].
• Antiplatelet agents. The decision to continue aspirin perioperatively is individualized based on cardiovascular and bleeding risks. The interruption of dual antiplatelet therapy (DAPT) requires careful multidisciplinary consultation due to the risk of stent thrombosis [31].
Standardized protocols, such as those derived from the PAUSE study, provide a robust framework for managing these complex scenarios [32].
Diagnosis and management of established perioperative VTE diagnosis
A high index of suspicion is paramount. D-dimer assays have limited utility in the postoperative period due to non-specific elevation. Compression duplex ultrasonography is the first-line diagnostic modality for suspected DVT, while computed tomography pulmonary angiography (CTPA) is the gold standard for diagnosing PE [33].
Initial treatment
• Initial anticoagulation. LMWH or fondaparinux are commonly used for initial treatment in hospitalized patients. For stable patients, DOACs are increasingly used either after a short course of parenteral therapy or as monotherapy, depending on the agent and clinical context [34].
• Duration of therapy:
▫ For a VTE provoked by major surgery, a minimum of 3 months of anticoagulation is standard [35].
▫ For unprovoked VTE, extended anticoagulation beyond 3 months may be considered based on the patient’s bleeding risk and preferences.
▫ For cancer-associated thrombosis (CAT), LMWH has been the traditional standard for at least 6 months, though certain DOACs (apixaban, rivaroxaban) are now validated alternatives in selected cancer patients with a low risk of bleeding [36].
Advanced interventions
• Catheter-directed thrombolysis (CDT) or pharmacomechanical thrombectomy may be considered for patients with massive iliofemoral DVT, severe symptoms, and a low bleeding risk, aiming to preserve valvular function and prevent post-thrombotic syndrome [37].
• Inferior vena cava (IVC) filters are reserved for patients with acute proximal DVT in whom therapeutic anticoagulation is contraindicated. Due to long-term risks of filter thrombosis and migration, retrievable filters should be removed once anticoagulation can be safely initiated [38].
Bleeding, reversal, and safety considerations
The use of perioperative anticoagulation inherently increases bleeding risk. Meticulous attention to dosing, timing, and renal function mitigates this risk.
Reversal agents:
• Protamine sulfate partially reverses UFH and, to a lesser extent, LMWH.
• Vitamin K and prothrombin complex concentrates (PCC) are used for warfarin reversal.
• Idarucizumab is a specific reversal agent for the direct thrombin inhibitor dabigatran [39].
• Andexanet alfa is approved for the reversal of factor Xa inhibitors (apixaban, rivaroxaban) in cases of life-threatening bleeding [40].
Institutional protocols for the management of anticoagulant-related bleeding are essential (Figure 7).

Figure 7. Thrombosis in rheumatological diseases. Source: Chapter 12, Thrombosis in Rheumatological Diseases. License: CC BY 4.0.
Peri-discharge and post-discharge considerations
Given that many VTE events occur after discharge, transition-of-care planning is vital. This includes prescribing extended-duration prophylaxis for indicated high-risk patients, ensuring patient education regarding the signs and symptoms of VTE and medication adherence, and clearly documenting the prophylaxis plan in the discharge summary.
Evidence summary and guideline highlights
• Validated risk assessment models, like the Caprini score, should form the foundation of prophylaxis decisions.
• LMWH is the standard pharmacologic agent in most general surgical settings.
• Mechanical prophylaxis is recommended when anticoagulants are contraindicated and as an adjunct in high-risk patients.
• Extended prophylaxis for 4 weeks is recommended after major cancer surgery of the abdomen and pelvis.
• DOACs are firmly established in orthopedic prophylaxis and VTE treatment, but their use for prophylaxis in general surgery requires careful patient selection (Table 5).
Table 7. Summary of major guideline
|
Guideline |
Year |
Key recommendations |
|---|---|---|
|
ACCP (9th ed.) |
2022 |
Risk-based prophylaxis, LMWH preferred, early ambulation. |
|
NICE (NG89) |
2021 |
Assess all surgical inpatients; LMWH or fondaparinux unless contraindicated. |
|
ASH guidelines |
2020 |
Prefer LMWH, discourage routine IVC filters, emphasize patient education. |
Controversies and gaps in evidence
• The optimal timing (preoperative vs. postoperative) of the first prophylactic dose for many general surgery procedures remains uncertain.
• Dosing strategies for special populations, particularly the morbidly obese and those with renal impairment, require further high-quality evidence.
• The role of DOACs for VTE prophylaxis across the spectrum of non-orthopedic general surgery needs clarification through large randomized controlled trials.
• The development of biomarkers or advanced predictive models beyond clinical scores could further refine individualized risk assessment [41].
Future directions and research priorities
1. Direct comparative trials of DOACs versus LMWH for extended prophylaxis following major abdominal surgery, particularly in oncology.
2. Studies to refine the indications and optimal duration of extended prophylaxis across diverse surgical subgroups.
3. Implementation science research focused on improving adherence to evidence-based VTE prophylaxis guidelines.
4. Development of integrated risk prediction models that incorporate both clinical variables and novel biomarkers.
Conclusions
The effective prevention and management of DVT in surgical patients demand a systematic approach. This includes structured risk assessment, the application of evidence-based prophylaxis tailored to individual thrombotic and bleeding profiles, and clear protocols for perioperative anticoagulation management. LMWH, combined with mechanical measures, remains foundational. Extended-duration prophylaxis is a key strategy in high-risk groups, especially following cancer surgery. While DOACs have revolutionized the treatment of VTE, special situations still necessitate the use of parenteral agents or highly individualized approaches. Future research should aim to clarify the role of DOACs in broader surgical prophylaxis and generate more sophisticated tools for personalized VTE prevention.
Author contributions
Muhammad Munir Memon, Zaheera Saadia ‒ critical review for scientific accuracy, editing of methodology and clinical content, and final approval of the manuscript.
Manar Mohammed Al Qapa, Hessah Abdulrahman Alkhudair, Modhi Saleh Alfraidi, Nouf Dalli Alenezi, Nouf Nawaf Alharbi, Maryam Mousa Alharbi, Lama Abdullah Alharbi, Wateen Mohammad Alharbi, Wafaa Abdulaziz Alhudithi ‒ conducted literature search, data extraction, drafting of the initial manuscript, preparation of tables and figures, and revision of the narrative review.
All authors have reviewed and approved the final version of the manuscript.
Ethical approval and informed consent
Since it’s a narrative review article, it does not require ethical approval from IRB.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Watson C, Saaid H, Vedula V, Cardenas JC, Henke PK, Nicoud F, Xu XY, Hunt BJ, Manning KB. Venous thromboembolism: Review of clinical challenges, biology, assessment, treatment, and modeling. Ann Biomed Eng 2024; 52(3): 467–486. DOI: 10.1007/s10439-023-03390-z.
2. Onwuzo C, Olukorode J, Sange W, Tanna SJ, Osaghae OW, Hassan A, Kristilere H, Orimoloye DA, Omokore O, Ganiyu B, Fayemi T, Addeh E. A review of the preventive strategies for venous thromboembolism in hospitalized patients. Cureus 2023; 15(11): e48421. DOI: 10.7759/cureus.48421.
3. Heit JA. Epidemiology of venous thromboembolism. Nat Rev Cardiol 2015; 12(8): 464–474. DOI: 10.1038/nrcardio.2015.83.
4. Uzel K, Azboy I, Parvizi J. Venous thromboembolism in orthopedic surgery: Global guidelines. Acta Orthop Traumatol Turc 2023; 57(5): 192–203. DOI: 10.5152/j.aott.2023.23074.
5. Kalayci A, Gibson CM, Chi G, Yee MK, Korjian S, Datta S, Nafee T, Gurin M, Haroian N, Qamar I, Hull RD, Hernandez AF, Cohen AT, Harrington RA, Goldhaber SZ. Asymptomatic deep vein thrombosis is associated with an increased risk of death: Insights from the APEX trial. Thromb Haemost 2018; 118(12): 2046–2052. DOI: 10.1055/s-0038-1675606.
6. Salous AK, Reyad A, Sweeney K, Mavanur A. A significant proportion of venous thromboembolism events in general surgical patients occurs after discharge: Analysis of the ACS-NSQIP essentials database. Perioper Med (Lond) 2019; 8: 18. DOI: 10.1186/s13741-019-0131-1.
7. Lurie JM, Png CYM, Subramaniam S, Marin M, Faries P. Virchow’s triad in “silent” deep vein thrombosis. J Vasc Surg Venous Lymphat Disord 2019; 7: 640–645. DOI: 10.1016/j.jvsv.2019.02.011.
8. Pastori D, Cormaci VM, Marucci S, Franchino G, Del Sole F, Capozza A, Fallarino A, Corso C, Valeriani E, Menichelli D, Pignatelli P. A comprehensive review of risk factors for venous thromboembolism: From epidemiology to pathophysiology. Int J Mol Sci 2023; 24(4): 3169. DOI: 10.3390/ijms24043169.
9. Wilson S, Chen X, Cronin MA, Dengler N, Enker P, Krauss ES, Laberko L, Lobastov K, Obi AT, Powell CA, Schastlivtsev I, Segal A, Simonson B, Siracuse J, Wakefield TW, McAneny D, Caprini JA. Thrombosis prophylaxis in surgical patients using the Caprini Risk Score. Curr Probl Surg 2022; 59(11): 101221. DOI: 10.1016/j.cpsurg.2022.101221.
10. Chahal R, Alexander M, Yee K, Jun CMK, Dagher JG, Ismail H, Riedel B, Burbury K. Impact of a risk-stratified thromboprophylaxis protocol on the incidence of postoperative venous thromboembolism and bleeding. Anaesthesia 2020; 75(8): 1052–1061. DOI: 10.1111/anae.15077.
11. Shoeb M, Fang MC. Assessing bleeding risk in patients taking anticoagulants. J Thromb Thrombolysis 2013; 35(3): 312–319. DOI: 10.1007/s11239-013-0899-7.
12. Patel P, Varacallo MA. Low-Molecular-Weight Heparin (LMWH). StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing, 2025.
13. Robertson L, Strachan J. Subcutaneous unfractionated heparin for the initial treatment of venous thromboembolism. Cochrane Database Syst Rev 2017; 2017(2): CD006771. DOI: 10.1002/14651858.CD006771.pub3.
14. Zhang Y, Zhang M, Tan L, Pan N, Zhang L. The clinical use of Fondaparinux: A synthetic heparin pentasaccharide. Prog Mol Biol Transl Sci 2019; 163: 41–53. DOI: 10.1016/bs.pmbts.2019.02.004.
15. Chen A, Stecker E, Warden BA. Direct oral anticoagulant use: A practical guide to common clinical challenges. J Am Heart Assoc 2020; 9(13): e017559. DOI: 10.1161/JAHA.120.017559.
16. Ageno W, Caramelli B, Donadini MP, Girardi L, Riva N. Changes in the landscape of anticoagulation: A focus on direct oral anticoagulants. Lancet Haematol 2024; 11(12): e938–e950.
17. Liu HZ, Liang J, Hu AX. The efficacy and safety of aspirin in preventing venous thrombosis in major orthopedic surgery: An updated meta-analysis of randomized controlled trials. Medicine (Baltimore) 2023; 102(42): e35602. DOI: 10.1097/MD.0000000000035602.
18. Bartlett MA, Mauck KF, Stephenson CR, Ganesh R, Daniels PR. Perioperative venous thromboembolism prophylaxis. Mayo Clin Proc 2020; 95(12): 2775–2798.
19. Minze MG, Kwee YY, Hall RG II. Low-molecular-weight heparin prophylaxis dosing: Is weight an issue? J Pharm Technol 2015; 32(2): 75–80. DOI: 10.1177/8755122515617200.
20. Noureldin A, Ivankovic V, Delisle M, Wang TF, Auer RC, Carrier M. Extended-duration thromboprophylaxis following major abdominopelvic surgery – for everyone or selected cases only? Thromb Res 2024; 235: 175–180. DOI: 10.1016/j.thromres.2024.01.026.
21. Agnelli G. Prevention of venous thromboembolism in surgical patients. Circulation 2004; 110(24 Suppl 1): IV4–IV12. DOI: 10.1161/01.CIR.0000150639.98514.6c.
22. Herring B, Lowen D, Ho P, Hodgson R. A systematic review of venous thromboembolism mechanical prophylaxis devices during surgery. Langenbecks Arch Surg 2023; 408(1): 410. DOI: 10.1007/s00423-023-03142-6.
23. Helms J, Middeldorp S, Spyropoulos AC. Thromboprophylaxis in critical care. Intensive Care Med 2022; 49(1): 75–78. DOI: 10.1007/s00134-022-06850-7.
24. Sobieraj DM, Coleman CI, Tongbram V, Chen W, Colby J, Lee S, Kluger J, Makanji S, Ashaye A, White CM. Comparative effectiveness of combined pharmacologic and mechanical thromboprophylaxis versus either method alone in major orthopedic surgery: A systematic review and meta-analysis. Pharmacotherapy 2013; 33(3): 275–283. DOI: 10.1002/phar.1206.
25. Wang Z, Yu Z, Niu T. Prolonged duration of pharmacological thromboprophylaxis following oncologic surgery: A systematic review and meta-analysis of RCTs. Thromb Res 2025; 255: 109500. DOI: 10.1016/j.thromres.2025.109500.
26. Carvalho L, Almeida RF, Nora M, Guimarães M. Thromboembolic complications after bariatric surgery: Is the high risk real? Cureus 2023; 15(1): e33444. DOI: 10.7759/cureus.33444.
27. Wang S, Wu L. Risk factors for venous thrombosis after spinal surgery: A systematic review and meta-analysis. Comput Math Methods Med 2022; 2022: 1621106. DOI: 10.1155/2022/1621106.
28. Tseng E. Clarifying indications and dosing of anticoagulants in pregnancy. Hematologist 2023; 20(1). DOI: 10.1182/hem.V20.1.202317.
29. Barnes GD, Douketis JD, Spyropoulos AC. Perioperative management of DOACs: Key points. JAMA 2024.
30. Douketis JD, Spyropoulos AC, Murad MH, Arcelus JI, Dager WE, Dunn AS, Fargo RA, Levy JH, Samama CM, Shah SH, Sherwood MW, Tafur AJ, Tang LV, Moores LK. Perioperative management of antithrombotic therapy: An American College of Chest Physicians clinical practice guideline. Chest 2022; 162(5): E207–E243.
31. Premji AM, Blegen MB, Corley AM, Ulloa J, Booth MS, Begashaw M, Larkin J, Shekelle P, Girgis MD, Maggard-Gibbons M. Dual antiplatelet management in the perioperative period: Updated and expanded systematic review. Syst Rev 2023; 12(1): 197. DOI: 10.1186/s13643-023-02360-9.
32. Douketis JD, Spyropoulos AC, Anderson JM, Arnold DM, Bates SM, Blostein M, Carrier M, Caprini JA, Clark NP, Coppens M, Dentali F, Duncan J, Gross PL, Kassis J, Kowalski S, Lee Ay, Le Gal G, Le Templier G, Li N, MacKay E, Shah V, Shivakumar S, Solymoss S, Spencer FA, Syed S, Tafur AJ, Vanassche T, Thiele T, Wu C, Yeo E, Schulman S. The perioperative anticoagulant use for surgery evaluation (PAUSE) study: Design and rationale. Thromb Haemost 2017; 117(12): 2415–2424. DOI: 10.1160/TH17-08-0553.
33. Cox C, Roberts LN. Basics of diagnosis and treatment of venous thromboembolism. J Thromb Haemost 2025; 23(2): e01009. DOI: 10.1016/j.jtha.2025.01.009.
34. Leentjens J, Peters M, Esselink AC, Smulders Y, Kramers C. Initial anticoagulation in patients with pulmonary embolism: Thrombolysis, unfractionated heparin, LMWH, fondaparinux, or DOACs? Br J Clin Pharmacol 2017; 83(11): 2356–2366. DOI: 10.1111/bcp.13340.
35. Kearon C, Akl EA. Duration of anticoagulant therapy for deep vein thrombosis and pulmonary embolism. Blood 2014; 123(12): 1794–1801. DOI: 10.1182/blood-2013-12-512681.
36. Shah S, Karathanasi A, Revythis A, Ioannidou E, Boussios S. Cancer-associated thrombosis: A new light on an old story. Diseases 2021; 9(2): 34. DOI: 10.3390/diseases9020034.
37. Tang T, Chen L, Chen J, Mei T, Lu Y. Pharmacomechanical thrombectomy versus catheter-directed thrombolysis for iliofemoral deep vein thrombosis: A meta-analysis of clinical trials. Clin Appl Thromb Hemost 2019; 25: 1076029618821190. DOI: 10.1177/1076029618821190.
38. DeYoung E, Minocha J. Inferior vena cava filters: Guidelines, best practice, and expanding indications. Semin Intervent Radiol 2016; 33(2): 65–70. DOI: 10.1055/s-0036-1581088.
39. Aldhaeefi M, Badreldin HA, Alsuwayyid F, Alqahtani T, Alshaya O, Al Yami MS, Saleh KB, Al Harbi SA, Alshaya AI. Practical guide for anticoagulant and antiplatelet reversal in clinical practice. Pharmacy (Basel) 2023; 11(1): 34. DOI: 10.3390/pharmacy11010034.
40. Favresse J, Hardy M, van Dievoet MA, Sennesael AL, Douxfils J, Samama CM, Vornicu O, Dincq AS, Lessire S, Mullier F. Andexanet alfa for the reversal of factor Xa inhibitors. Expert Opin Biol Ther 2019; 19(5): 387–397. DOI: 10.1080/14712598.2019.1599355.
41. Zhao Q, Zhang C, Zhang W, Zhang S, Liu Q, Guo Y. Applications and challenges of biomarker-based predictive models in proactive health management. Front Public Health 2025; 13: 1633487. DOI: 10.3389/fpubh.2025.1633487.