Lietuvos chirurgija ISSN 1392–0995 eISSN 1648–9942
2026, vol. 25(2), pp. 124–140 DOI: https://doi.org/10.15388/LietChirur.2026.25(2).2
Clinical Profile and Therapeutic Approaches for Gastric Lipoma: A Comprehensive Scoping Review
Sajad Ahmad Salati
Qassim University, Department of Surgery, College of Medicine, Saudi Arabia
E-mail: s.salati@qu.edu.sa
https://orcid.org/0000-0003-2998-7542
https://ror.org/01wsfe280
Mohammad AlFehaid
Qassim University, Department of Surgery, College of Medicine, Saudi Arabia
E-mail: m.alfehaid@qu.edu.sa
https://orcid.org/0000-0003-0435-3260
https://ror.org/01wsfe280
Abstract. Background. Due to improvements in diagnostic imaging and the popularity of bariatric surgery, gastric lipoma (GL), a rare benign mesenchymal tumor, is becoming more widely recognized. Though open surgery has been the conventional method of management, the therapeutic scenario has changed considerably in the past ten years. Objective. This scoping review intends to delineate the clinical features, diagnostic findings, and the management trends for gastric lipomas that were documented between 2016 and 2025. Methods. A systematic search was carried out across many databases in accordance with PRISMA-ScR criteria. Eligible studies included case reports and series focusing on benign GLs in adult patients. Data extraction focused on demographics, symptomatology, tumor size, diagnostic modalities, and surgical outcomes. Results. A total of 33 articles describing 35 cases were included. For cases with available demographic data, the median age was 63 years (range: 17–85), with a 2.5:1 male predominance. The most common presentation was gastrointestinal bleeding (68.6%), followed by gastric outlet obstruction (20.0%). Larger tumor size was generally related to symptomatic presentation in the reviewed literature; notably, all reported “giant” lesions (>4 cm) were symptomatic. The most common diagnostic methods were esophagogastroduodenoscopy (91.4%) and CT (80.0%). There was an apparent shift toward less invasive treatments, such as laparoscopic (20.0%), robotic (5.7%), and endoscopic (17.1%) procedures, all of which had successful results. Conclusion. In published cases, gastric lipomas >4 cm were predominantly symptomatic and necessitated intervention. There is a clear trend toward minimally invasive and parenchyma-sparing techniques. The absence of long-term follow-up data, however, continues to be a major knowledge gap. Furthermore, the development of prospective multi-institutional registries is crucial to better define the natural history and intervention thresholds for this disorder, since asymptomatic giant lesions are probably underestimated because of publication bias.
Keywords: gastric lipoma, scoping review, minimally invasive surgery, endoscopic submucosal dissection, gastrointestinal bleed, gastric outlet obstruction.
Received: 2026-01-26. Accepted: 2026-02-12.
Copyright © 2026 Sajad Ahmad Salati, Mohammad AlFehaid. Published by Vilnius University Press. This is an Open Access article distributed under the terms of the Creative Commons Attribution Licence, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction
Gastric lipomas (GL) are rare, benign mesenchymal tumors, accounting for less than 1% of all gastric neoplasms and approximately 5% of all gastrointestinal lipomas [1]. Historically, these lesions were considered clinical curiosities, with the peer-reviewed English literature documenting only about 250 cases prior to the last decade [1, 2]. However, the increasing number of bariatric procedures and the widespread use of high-resolution computed tomography (CT) for diagnostic purposes in recent years, have led to incidental discovery of these lesions and contributed to the increase in their reported incidence [1, 2].
Most GLs originate in the submucosal layer and remain asymptomatic when small. However, clinical complications ‒ including abdominal pain, ulceration, overt gastrointestinal (GI) bleeding, and gastric outlet obstruction (GOO), typically arise once lesions exceed a diameter of 2–4 cm [3]. Lesions larger than 4 cm, categorized as “giant” gastric lipomas, are exceptionally rare and often present significant management challenges [1].
Currently, there are no established “gold-standard” protocols for the management of large symptomatic GLs [4]. While traditional open surgical excision was the historical mainstay, the last decade has seen a rapid emergence of minimally invasive techniques, such as laparoscopic resections and endoscopic submucosal dissection (ESD). Despite these technological developments, there is a notable lack of synthesized evidence regarding the safety, long-term outcomes, and the specific size thresholds that necessitate intervention in the contemporary era.
This scoping review aims to map the clinical characteristics, diagnostic findings, and the management trends for gastric lipomas reported between 2016 and 2025. By synthesizing contemporary case data, this review seeks to identify current knowledge gaps, particularly regarding longitudinal follow-up, and provide a framework for future prospective research and management algorithms.
Materials and methods
Study design. This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines. This framework ensured a transparent, systematic, and reproducible mapping of the clinical landscape regarding gastric lipomas over the last decade.
Selection of sources of evidence. A systematic search was performed by the authors independently across multiple electronic databases, including PubMed, Google Scholar and Scopus, for articles published between January 2016 and January 2025. The search strategy employed terms such as “gastric lipoma”, “submucosal gastric tumor”, and “benign gastric tumor”. Following a primary search in July 2025, a final update was conducted on August 20, 2025.
Inclusion and exclusion criteria:
• Inclusion. Case reports and series of adult patients with a histologically confirmed diagnosis of benign gastric lipoma.
• Exclusion. Non-English publications, literature reviews, studies lacking primary clinical data, and cases involving malignant variants such as liposarcomas.
Data charting process. Data extraction was guided by a customized checklist developed according to PRISMA-ScR guidelines to ensure standardized and comprehensive variable collection. For each included case, data were extracted and organized into two primary tables (Table 1 and Table 2) covering eight key variables:
• Patient demographics. Age and gender.
• Clinical profile. Presentation/symptomatology and comorbidities.
• Diagnostics. Endoscopy (EGD), CT imaging, and endoscopic ultrasound (EUS) findings.
• Management. Therapeutic approach (surgical vs. non-surgical), intraoperative findings, and histopathology.
• Outcomes. Postoperative clinical course and longitudinal follow-up data.
Critical appraisal of individual sources of evidence. In alignment with the objectives of a scoping review to map available evidence rather than provide a graded meta-analysis, the methodological quality was assessed based on the completeness of clinical and management variables. While formal risk-of-bias tools for randomized trials were not applicable due to limited data, the review acknowledges the inherent limitations of case-report data, including selection and publication bias, which may over-represent high-acuity or symptomatic “giant” lesions (>4 cm) compared to the general population.
Synthesis of results. Data were synthesized using descriptive statistics. Continuous variables, such as patient age and tumor size, are presented as medians and ranges (or interquartile ranges), while categorical variables, such as clinical symptoms and surgical techniques, are expressed as frequencies and percentages. Due to the heterogeneous nature of the case-report data, inferential statistical testing was not performed. The results are further illustrated through a PRISMA-ScR flow diagram (Figure 1) and trend mapping of management shifts (Figure 3).
Results
Study selection. The initial systematic search across PubMed, EMBASE, Web of Science Core Collection and Scopus yielded a total of 81 records. After the removal of 42 duplicate entries, 39 unique records underwent title and abstract screening. Of these, 36 reports were sought for full-text retrieval and assessed for eligibility. Three articles were subsequently excluded: one was inaccessible, one lacked sufficient clinical management data, and one was excluded upon histopathological review revealing a malignant variant. Ultimately, 33 studies meeting all inclusion criteria were selected, representing a total of 35 distinct clinical cases of gastric lipoma for qualitative synthesis (Figure 1).
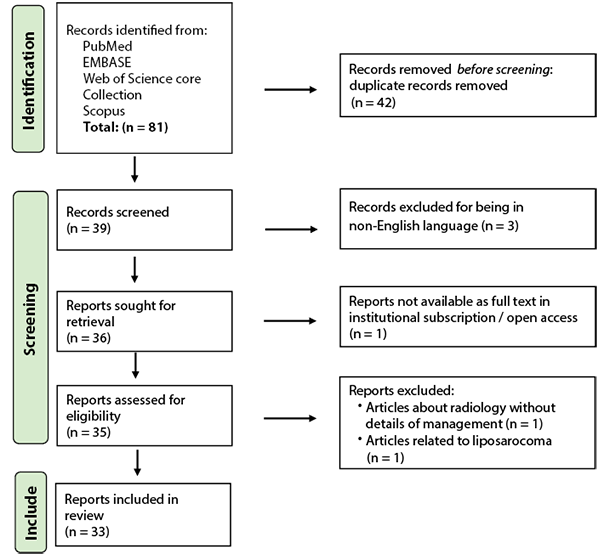
Figure 1. PRISMA-ScR flow diagram of the study selection process for gastric lipoma case reports (2016–2025)
Demographics and clinical presentation. The demographic profile of the 35 cases revealed a median age of 63 years (range: 17–85 years). A notable male predominance was observed, with 25 males (71.4%) compared to 10 females (28.6%).
The clinical presentations were categorized as follows:
• Gastrointestinal bleeding. The most prevalent symptom, occurring in 24 cases (68.6%) as melena or hematemesis.
• Gastric outlet obstruction (GOO). This was documented in 7 patients (20.0%).
• Asymptomatic/incidental. Three patients (8.6%) had no symptoms, including 2 (5.7%) cases detected during preoperative evaluation for bariatric surgery.
• Other. Dyspepsia was reported in one case (2.9%), and one atypical case (2.9%), had glycemic variability, with alternating hypoglycemic and hyperglycemic episodes alongside obstructive symptoms.
Twenty-one patients (60%) had comorbidities; the most common disorders were hypertension, dyslipidemia, coronary artery disease, chronic renal disease, morbid obesity, and gastroesophageal reflux disease (GERD).

Figure 2. Clinical presentation of gastric lipomas
Diagnostic findings. The diagnostic workup primarily utilized the following modalities:
• Esophagogastroduodenoscopy (EGD). Performed in 91.4% of cases.
• Computed tomography (CT). Performed in 80.0% of cases, typically showing a well-circumscribed mass with fat density.
• Endoscopic ultrasound (EUS). Utilized in 40.0% of cases.
• MRI. Employed in only a single case (2.9%).
Lesion size ranged from 1.3 to 17 cm, with a median size of 6.0 cm. Notably, all reported “giant” gastric lipomas (>4 cm) were associated with clinical symptoms. The most frequent anatomical site was the antrum (68.6%).
Management and technological shift. Management strategies were predominantly surgical, but demonstrated a shift toward minimally invasive techniques:
• Surgical intervention. 26 patients (74.3%) underwent operative management. While laparotomy remained the most common (48.6%), there was significant use of laparoscopic (20.0%) and robotic-assisted (5.7%) approaches.
• Endoscopic intervention. Endoscopic submucosal dissection (ESD) or excision was used in 20.0% of cases.
• Conservative management. Only 2 cases (5.7%) were managed non-operatively with PPIs or Helicobacter pylori eradication.
Outcomes and follow-up. Histopathological examination confirmed the diagnosis of benign gastric lipoma in all 35 cases. The postoperative phase was uneventful across the entire cohort, with no reported mortality or significant complications. However, longitudinal data remains a significant gap:
• Follow-up availability. This was clearly documented for only 16 cases (45.7%).
• Duration. The mean follow-up was 6.9 months, with fewer than 10% of total cases reporting outcomes beyond one year.
• Recurrence. No instances of tumor recurrence were reported during the monitored periods.
Table 1. Patient characteristics (demographics, clinical presentation and diagnostic investigations)
|
S. no. |
Series/year |
Age (years)/ gender |
Clinical |
Comorbidities |
Esophagogastroduodenoscopy (EGD) |
Imaging |
Imaging |
|---|---|---|---|---|---|---|---|
|
1. |
Nasa et al. / 2016 [5] |
56/F |
AP, ES, NV, PPF for 1 year. |
None |
Smooth bulge in the gastric antrum (5 cm) with normal mucosa. |
A homogeneous, hyperechoic SML. |
A 6 cm homogeneous, antro-pyloric, oval mass with fatty density. |
|
2. |
Al Shammari et al. / 2016 [6] |
41/M |
Asymptomatic, detected incidentally during evaluation for BSO. |
Morbid obesity |
A rounded 3×3 cm antral mass with normal mucosa, with positive “cushion-sign” and “tenting sign”. |
‒ |
A 3.5×3 cm, oval, antral fatty lesion. |
|
3. |
Aoyama et al. / 2017 [7] |
54/M |
AP (Epigastric) and melena. |
On F/U of gastric SMT for 8 years |
A SML with ulcer on the anterior wall of the lower gastric body. |
Hyperechoic SML, antral extending to gastric body. |
A fatty mass spanning entire gastric wall of the antrum and gastric body, except LC. |
|
4. |
Ichinose et al. / 2017 [8] |
66/M |
Asymptomatic SML in the gastric antrum with recent increase in size. |
Dyslipidaemia, DM, under F/U of gastric lesion for 10 years |
An antral mass with reddish mucosa and ulcer; negative cushion sign. |
A 1.3 cm homogeneous, hyperechoic, antral SML. |
Mucosal thickening in the PGW (antrum). |
|
5. |
Termos et al. / 2017 [9] |
62/M |
PPF and weight loss for 6 months, an episode of hematemesis and syncope. |
HT |
A large SML extending from GEJ to pylorus along LC with a 4 cm linear ulcer. |
‒ |
A 17×9×8 cm well-defined oval SML of fatty density arising from PGW. |
|
6. |
Cappell et al. / 2017 [1] |
63/M |
ES and weight loss for 6 months; melena and ED for 3 days. |
HT, dyslipidaemia |
A 13 cm wide, antral SML with smooth mucosa and focal ulceration. |
‒ |
Well-circumscribed, uniform 13.4×8.4×8.2 cm mass, with fatty attenuation. |
|
7. |
Cappell et al. / 2017 [1] |
78/F |
Melena with orthostatic dizziness for 3 days. |
HT, AF, CKD, dyslipidaemia |
An antral SML, focally ulcerated, with a positive cushion sign. |
‒ |
A 9.5×6.0×4.5 cm, antral SML. |
|
8. |
Amundson et al. / 2018 [10] |
58/M |
AP, NV and melena. |
HT, an incidental gastric lesion in CT scan for 5 years |
A large, fundal SML with stigmata of recent bleeding. |
An oval, isoechoic SML in the fundus 9x5 cm with well-defined borders. |
Interval increase in size of the fatty gastric lesion from 3 cm to 7.2×10.3×7.3 cm in 7 years. |
|
9. |
Krishnaraj et al. / 2018 [11] |
80/F |
AP for 2 months; haematemesis and melena for 1 day. |
CAD |
A smooth bulge in the posterior antral wall with an ulcer. |
‒ |
An 8×3 cm SML in PGW (antrum) with uniform fat density (–70 HU). |
|
10. |
Abdulrahman et al. / 2018 [12] |
65/M |
NV and dysphagia. |
CVA |
Features of GOO with no intraluminal mass or ulceration. |
‒ |
A pyloric SML, 4.5x8 cm, with a fat density. |
|
11. |
Ingason et al. / 2018 [13] |
55/M |
Chronic heartburn, PPF, ES. |
GERD, bronchial asthma |
A yellowish tumor causing GOO during peristalsis. |
‒ |
A large antral mass with uniform adipose density. |
|
12. |
Sharayah et al. / 2019 [14] |
85/M |
AP (epigastrium), ES, NV, weight loss for 3 months. |
Anaemia |
A large antral mass with friable ulcer causing GOO. |
‒ |
Homogeneous, antral, 5x2.5 cm, SML with fat density. |
|
13. |
Agafonoff et al. / 2019 [15] |
58/F |
Asymptomatic, detected incidentally during evaluation for BSO. |
Morbid obesity |
A 3 cm, SML at LC with a positive pillow sign. |
A 3.3x1.6 cm echogenic, SML at LC. |
A well-circumscribed, smooth, ovoid SML of uniform fat attenuation, 1.5×1.5×3.0 cm, at LC. |
|
14. |
Mir et al. / 2020 [16] |
67/M |
Upper GI bleed. |
On F/U for asymptomatic GL for 2 years, HH |
A 5 cm gastric antral SML, ulcerated, at IA with a positive “cushion” sign. |
A hyperechoic SML. |
‒ |
|
15. |
Sabbah et al. / 2020 [17] |
40/M |
Episode of hematemesis. |
None |
A 4 cm, ulcerated, antral yellowish SML with a positive pillow sign. |
A 4 cm hyperechoic SML. |
A well-circumscribed hypodense antral SML. |
|
16. |
Kumar et al. / 2021 [18] |
54/M |
Episode of massive hematemesis. |
None |
‒ |
‒ |
A 5 cm, well-circumscribed antral SML with fatty density (−90 HU). |
|
17. |
Lalanda et al. / 2021 [19] |
79/M |
Massive upper GI bleed with melena. |
CAD, AF |
An ulcerated, antral SML. |
A hyperechoic SML measuring 9×4 cm. |
A well-encapsulated, antral, 6.2×3.3 cm, SML, with fat density (−90 HU). |
|
18. |
Solis et al. / 2021 [20] |
54/M |
NV and cough for 3 weeks. |
None |
Antral gastritis, a SML in the distal body, with a positive “pillow sign”. |
‒ |
‒ |
|
19. |
Parreira et al. / 2021 [21] |
60/F |
Postprandial AP, NV for 6 months and hematemesis (once). |
DM, CAD, obesity, dyslipidaemia |
A soft, semi-circumferential, antral SML. |
A homogeneous, hyperechoic SML. |
An 8×3 cm, well-encapsulated, fat-attenuated SML in PGW (antrum) causing GOO. |
|
20. |
Rezaii et al. / 2021 [22] |
38/M |
AP, NV, melena and hematemesis for 2 months. |
None |
A large, antral SML causing GOO. |
A well-defined, heterogeneous, antral, 4.4x4.1 cm SML. |
‒ |
|
21. |
Marques et al. / 2022 [23] |
73/F |
Sudden loss of consciousness. |
Depression, dementia |
‒ |
‒ |
An antral, ulcerated fatty SML, 6×4.4×4.1 cm with bleeding. |
|
22. |
Nabi et al. / 2022 [24] |
? /M |
Intermittent GOO symptoms. |
None |
A 6 cm, pedicled, antral SML causing GOO. |
‒ |
‒ |
|
23. |
Al-Janabi et al. / 2023 [25] |
66/M |
AP (epigastrium) and reflux. |
None |
A 3 cm, antral SML. |
‒ |
‒ |
|
24. |
Martins et al. / 2023 [26] |
63/M |
ES, dyspepsia, and one episode of melena. |
HT, DM, h/o carotid endarterectomy and appendectomy |
A 7 cm, ulcerated, antral SML. |
‒ |
A homogeneous, antral, SML 8.8x4.3 cm, with fat density. |
|
25. |
Al-Anbagi et al. / 2024 [27] |
60/M |
Melena for 5 days; AP, fatigue, and orthostatic dizziness for 3 days. |
None |
A 7 cm SML at cardia (below GEJ), causing partial obstruction. |
A 5.3x39 cm homogenous, hyperechoic SML. |
A fatty SML (6.5x6.2x5.4 cm) in gastric fundus and cardia. |
|
26. |
Chaouch et al. / 2024 [28] |
50/F |
Multiple episodes of melena. |
None |
A 5 cm, prepyloric with a 1 cm ulcer. |
‒ |
A SML hanging from LC, 3.8 cm, with homogeneous fat density. |
|
27. |
Cherif et al. / 2024 [2] |
39/M |
PA (epigastric) with hematemesis for 1 week. |
None |
An antral, SML with an ulcer. |
‒ |
A heterogeneous, antropyloric, 6x5 cm, SML with fat density. |
|
28. |
Jarrett et al. / 2024 [29] |
67/M |
Multiple episodes of melena for 1 week. |
HT, CF, COPD |
A 5 cm SML, along GC with a 1 cm ulcer. |
‒ |
A 4.5 cm antral wall fat density. |
|
29. |
66/M |
NV, hematemesis and melena for 5 days. |
HT, DM, GERD, diverticulosis |
An ulcerated SML with attachments in antrum and duodenal bulb. |
‒ |
An 8.9×2.8×5.4 cm fat density SML. |
|
|
30. |
Qadir et al. / 2024 [30] |
64/M |
Syncope and hematemesis. |
GERD |
A 7 cm ulcerated SML at LC extending into the gastric antrum, pre-pylorus, and pyloric region. |
An antral SML. |
A distal gastric 7.4x4 cm, heterogenous mass with fat-like density. |
|
31. |
Rasmussen et al. / 2024 [31] |
? /F |
Melena with EB for 5 days. |
Treated thyroid cancer, cholecystectomy |
Distal gastric SML with stigmata of recent haemorrhage. |
Antral SML. |
Large antral SML with fat like density. |
|
32. |
Setake et al. / 2024 [32] |
62/F |
AP (epigastric) for 1 month, melena for 3 days. |
On F/U of 1 cm gastric lipoma for 7 years |
A 4 cm antral SML with ulceration but no active hemorrhage. |
‒ |
An antral SML partially solid with uniform fat density. |
|
33. |
Thomas et al. / 2024 [33] |
65/F |
AP, PPF, and glycaemic variability for 3 years. |
None |
Pyloric SML acting like a ball-valve. |
‒ |
A homogenous, oval, 1.6x0.8 cm, pyloric mass with a density of –60 HU, prolapsing into pyloric canal. |
|
34. |
Joshi et al. / 2025 [34] |
69/M |
ED, melena, PPP (periumbilical). |
CKD, CAD, DM, Barrett’s esophagus |
A 4×4 cm SML with a large adherent clot and ulceration in the distal gastric corpus. |
‒ |
‒ |
|
35. |
Wang et al. / 2025 [4] |
17/F |
PPF, NV for |
None |
A 7x8 cm, smooth SML in gastric body, causing GOO. |
A hyperechoic SML with well-defined margins. |
A homogeneous fat-density SML. |
|
SML ‒ submucosal lesion; HT – hypertension; IHD – ischemic heart disease; CAD ‒ coronary artery disease; CKD – chronic kidney disease; AF – atrial fibrillation; GI – gastrointestinal; HU ‒ Hounsfield units; CF ‒ cardiac failure; COPD ‒ chronic obstructive pulmonary disease; HH ‒ hereditary hemochromatosis; GERD – gastroesophageal reflux disease; CVA ‒ cerebrovascular accident; GOO ‒ gastric outlet obstruction; F/U ‒ follow-up; GEJ ‒ gastroesophageal junction; LC ‒ lesser curvature; GC – greater curvature; IA ‒ incisura angularis; PGW ‒ posterior gastric wall; AP ‒ abdominal pain; ES – early satiety; NV – nausea and vomiting; PPF – postprandial fullness; PPP – postprandial pain; ED ‒ exertional dyspnoea; BSO ‒ bariatric surgical operation. |
|||||||
Table 2. Patient characteristics (management and outcomes)
|
S. no. |
Series/year of publication |
Management |
Operative findings |
Histo-pathological examination |
Postoperative phase |
Follow-up |
|---|---|---|---|---|---|---|
|
1. |
Nasa et al. / 2016 [5] |
LRT, TAG & excision of lipoma. |
A soft tumour with well-defined margins along the LC of the stomach. |
Mature, well-differentiated adipocytes. |
U |
Asymptomatic at 6 months. |
|
2. |
Al Shammari et al. / 2016 [6] |
LAP, SMR of lipoma during SG. |
An ovoid, well circumcised mass measuring 4×3×2 cm. |
Mature adipose tissue separated into lobules by fibrovascular septae. |
U |
Patient doing well at 2 weeks. |
|
3. |
Aoyama et al. / 2017 [7] |
LRT with TG. |
Smooth and diffusely elevated mucosal surface with an ulcer along GC. |
Mature adipocytes without nuclear atypia replacing the gastric submucosal and muscle layers. |
U |
No recurrence. |
|
4. |
Ichinose et al. / 2017 [8] |
ESD. |
‒ |
Mature fat tissue with a clear border. |
U |
‒ |
|
5. |
Termos et al. / 2017 [9] |
LRT with TAG and enucleation of lipoma. |
Stomach appeared to be thin with a huge SML with an overlying ulcer. |
A giant mural benign lipoma with mucosal inflammation. |
U |
Asymptomatic with normal endoscopy at 6 months. |
|
6. |
Cappell et al. / 2017 [1] |
LRT with PG extended by PBD and Billroth II reconstruction. |
Homogeneous, soft, SML, 14.5×8.7×7.5 cm mass. |
Features of benign lipoma. |
U |
Asymptomatic at 8 weeks. |
|
7. |
LRT, DG. |
SML, 9.0×6.0×4.5 cm. |
Features of benign lipoma. |
U |
‒ |
|
|
8. |
Amundson et al. / 2018 [10] |
LRT with TAG and excision of the lipoma. |
Soft, fleshy mass, 12 cm in size. |
A submucosal well circumscribed, non-encapsulated mass of mature adipose tissue without atypia or mitotic figures. |
U |
Asymptomatic at 3 weeks. |
|
9. |
Krishnaraj et al. / 2018 [11] |
LRT with TAG and excision of gastric mass. |
A soft lobulated swelling in the posterior gastric wall with ulcerated mucosa. |
Features of benign lipoma. |
U |
Asymptomatic and no recurrence at 2 years. |
|
10. |
Abdulrahman et al. / 2018 [12] |
LRT, excision of antral mass and gastrostomy. |
Intraluminal gastric tumor arising from the submucosal layer of antrum. |
Mature adipocytes without cytological atypia, arranged in lobules. |
U |
‒ |
|
11. |
Ingason et al. / 2018 [13] |
ESD. |
‒ |
A 7x3 cm, well-circumscribed, benign lipoma, surrounded by a fibrous capsule. |
U |
Endoscopy at 4 months revealed a normal-looking pylorus, well-healed resection plane and no recurrence. |
|
12. |
Sharayah et al. / 2019 [14] |
ESD. |
‒ |
Features of benign lipoma. |
U |
Endoscopy at 4 weeks revealed a well-healed scar; asymptomatic at 12 week. |
|
13. |
Agafonoff et al. / 2019 [15] |
LAP, SMR of lipoma during SG. |
‒ |
Benign lipoma. |
U |
Doing well at 3 months. |
|
14. |
Mir et al. / 2020 [16] |
ESD. |
A yellow-coloured 7 cm submucosal lesion at antrum. |
Features of benign lipoma. |
U |
‒ |
|
15. |
Sabbah et al. / 2020 [17] |
LRT, PG. |
‒ |
Submucosal lipoma and ulceration of the overlying mucosa. |
U |
‒ |
|
16. |
Kumar et al. / 2021 [18] |
LAP, TAG and wedge resection of stomach. |
Tumour arising from the posterior gastric wall. |
Features of benign lipoma. |
U |
Symptom free at 10 month. |
|
17. |
Lalanda et al. / 2021 [19] |
LRT, TAG with tumour enucleation. |
Tumour arising from the posterior antral wall. |
Features of submucosal lipoma with 9.5×4.8×2.5 cm and ulceration. |
U |
No recurrence. |
|
18. |
Solis et al. / 2021 [20] |
CON, PPIs. |
‒ |
Random mucosal biopsies displayed a positive “naked fat sign”; HPE showed antral/oxyntic mucosa with minimal chronic gastritis. |
‒ |
Symptom free. |
|
19. |
Parreira et al. / 2021 [21] |
LRT, TAG with tumour enucleation. |
Large, mobile, soft, globular antral mass. |
Features of an 80×35×35 mm lipoma. |
U |
Symptom free, no recurrence at 18 months. |
|
20. |
Rezaii et al. / 2021 [22] |
LRT, PG. |
A yellowish, smooth, sub-serosal 5 cm antral mass. |
A submucosal well-defined gastric lipoma. |
U |
‒ |
|
21. |
Marques et al. / 2022 [23] |
LRT, STG. |
‒ |
Gastric lipoma with steatonecrosis, in the submucosal and muscular layers. |
U |
‒ |
|
22. |
Nabi et al. / 2022 [24] |
ESD using a bipolar radiofrequency device. |
‒ |
A submucosal well-defined benign gastric lipoma. |
U |
‒ |
|
23. |
Al-Janabi et al. / 2023 [25] |
LRT, STG. |
Soft, antral mass, 3 cm in size. |
Benign, well-circumscribed adipose tissue in the submucosa with normal overlying mucosa. |
U |
Symptom free, no recurrence at 6 months. |
|
24. |
Martins et al. / 2023 [26] |
LAP, PAG and enucleation of the lesion. |
Submucosal fatty lesion. |
Lesion 108.9 grams and measuring 9x6x3.5 cm, with features of benign lipoma. |
U |
Symptom free at 3 weeks. |
|
25. |
Al-Anbagi et al. / 2024 [27] |
ROB, GWR. |
‒ |
Benign lipoma. |
U |
‒ |
|
26. |
Chaouch et al. / 2024 [28] |
LAP, AG, and enucleation of lipoma. |
A 4 cm, pedunculated SML on the posterior wall of the prepyloric region. |
Benign lipoma. |
U |
Symptom free at 1 month. |
|
27. |
Cherif et al. / 2024 [2] |
LRT, DG. |
Antral tumour measuring 5x5 cm. |
A smooth submucosal yellow lobulated adipose mass. |
U |
‒ |
|
28. |
Jarrett et al. / 2024 [29] |
LAP, GWR. |
‒ |
A 7.0×4.0×2.8 mm partially encapsulated homogenous adipose tissue with focal areas of haemorrhage. |
U |
Symptom free at 6 weeks. |
|
29. |
LRT, AG with resection of SML. |
A gastroduodenal ulcerated mass. |
A 3×2.5×1.5 cm gelatinous lobulated yellow grey adipose mass. |
U |
‒ |
|
|
30. |
Qadir et al. / 2024 [30] |
ROB, DG with gastrojejunostomy. |
‒ |
Features consistent with lipoma. |
U |
‒ |
|
31. |
Rasmussen et al. / 2024 [31] |
LRT, DG (Billroth II). |
A 7x5x4 cm antral tumour. |
Fat cells with partial necrosis. |
U |
Symptom free and no recurrence at 2 years. |
|
32. |
Setake et al. / 2024 [32] |
LAP, DG. |
‒ |
Benign lipoma. |
U |
‒ |
|
33. |
Thomas et al. / 2024 [33] |
Endoscopic excision. |
‒ |
Benign lipoma. |
U |
At 2 years, asymptomatic and euglycemic. |
|
34. |
Joshi et al. / 2025 [34] |
CON, Helicobacter pylori eradication. |
‒ |
Benign lipoma. |
‒ |
No further episodes of melena, frank bloody stools, or hematemesis. |
|
35. |
Wang et al. / 2025 [4] |
ESD. |
‒ |
Benign gastric lipoma. |
U |
‒ |
|
ESD ‒ endoscopic submucosal dissection; LRT ‒ laparotomy; LAP ‒ laparoscopic; ROB – robotic; TAG ‒ transverse anterior gastrotomy; AG ‒ anterior gastrotomy; SMR ‒ submucosal resection; SG ‒ sleeve gastrectomy; TG ‒ total gastrectomy; PG ‒ partial gastrectomy; PBD ‒ partial bulbar duodenectomy; DG ‒ distal gastrectomy; STG ‒ subtotal gastrectomy; GWR ‒ gastric wedge resection; CON ‒ conservative treatment; LC ‒ lesser curvature; GC ‒ greater curvature; U ‒ uneventful; SML ‒ submucosal lesion; Postop ‒ postoperative. |
||||||
Discussion
Demographic and clinical mapping. The current scoping review maps the clinical landscape of gastric lipoma (GL) based on 35 cases, as summarized in Tables 1 and 2. The median age (63 years) and the 2.5:1 male-to-female ratio align with existing literature. Specifically, Cappell [1] reported a mean age of 54.5±17.0 years and a similar sex distribution in a review of 32 giant GL cases [1].
Upper gastrointestinal (UGI) bleeding, presenting as melena or hematemesis, was the most prevalent symptom in our cohort (68.6%). The pathophysiology of bleeding in GL is often attributed to venous stasis, mechanical friction against the gastric wall, or pressure-induced necrosis as the lesion outgrows its blood supply [1, 35‒37].
The incidental and longitudinal profile. A noteworthy finding in this mapping exercise is the detection of asymptomatic GLs (8.6%), particularly those identified during preoperative workups for bariatric surgery. As the volume of bariatric procedures increases globally, clinicians should anticipate a rise in incidental GL diagnoses. Furthermore, 14.3% of cases were previously known lesions that progressed to become symptomatic or increased in size. This highlight a critical “knowledge gap” regarding the natural history of GL; it is imperative to counsel patients on the potential for progression to ensure they are not lost to follow-up and to facilitate timely intervention.
Diagnostic modalities and pathognomonic signs. EGD remains the primary diagnostic tool (91.4%), followed by CT (80%) and Endoscopic ultrasound-EUS (40%). While MRI offers high sensitivity for fatty tissue ‒ revealing hyperintense signals on T1-weighted sequences that diminish with fat suppression ‒ it remains underutilized (2.9%).
On EGD, several pathognomonic signs can guide the clinician:
• Pillow/cushion sign. Indentation upon forceps compression [17, 33].
• Tenting sign. Easy retraction of the overlying mucosa [33, 37].
• Naked fat sign. Exposure of adipose tissue following biopsy [33, 37].
• Pot of gold sign. A distinct visual effect of microscopic lipid globules observed when the biopsy forceps penetrates the submucosal layer [38].
Radiologically, CT is nearly pathognomonic, showing well-circumscribed masses with low attenuation (70 to 120 Hounsfield Units). However, the presence of internal septa should prompt the exclusion of liposarcoma [39, 40].
Differential diagnosis and the role of Helicobacter pylori. The exclusion of malignancy, particularly liposarcoma, is vital. Liposarcomas often demonstrate higher densitometry on CT and require definitive diagnosis through MDM2 and CDK4 gene amplification analysis [41, 42]. Other differentials mapped in this review include GIST, metastatic deposits, and heterotopic pancreas.
An intriguing observation in our review is the potential role of Helicobacter pylori in ulcerated GL. As demonstrated by Joshi et al. [34], active Helicobacter pylori infection may exacerbate the risk of life-threatening bleeding in GL patients. This suggests that Helicobacter pylori screening and eradication should be integrated into the management protocol for ulcerated GL to improve outcomes.
Evolution of management: a decadal shift. Our review highlights a significant shift in the surgical landscape. While Cappell’s 2017 review reported a 90.6% laparotomy rate, our cohort shows a transition toward minimally invasive and endoscopic approaches. Laparotomy was utilized in only 48.6% of cases, with a rise in laparoscopic (20%), robotic (5.7%), and endoscopic submucosal dissection (ESD) (17.1%) techniques (Figure 3).

Figure 3. Trends in the management of gastric lipoma
Despite this shift toward less invasive methods, there were no reported recurrence or mortality. While the literature suggests a recurrence rate of <5% (usually due to incomplete capsule excision), none was observed in this cohort, further supporting the safety and efficacy of contemporary parenchyma-sparing techniques [10].
Future directions
1. Multi-institutional registries. The present database is primarily made up of individual case reports because gastric lipomas are still rare, which makes it difficult to develop high-level clinical guidelines. To compile uniform data on the natural history, diagnostic precision, and long-term consequences of these lesions, prospective, multi-institutional registries must be established. The creation of evidence-based management algorithms would be made easier by such registries, especially when it comes to figuring out the size threshold at which asymptomatic lesions need to be treated.
2. Artificial intelligence (AI) in diagnostics. AI algorithms are anticipated to be developed to distinguish between benign lipomas and potentially pre-malignant gastrointestinal stromal tumors (GISTs) by analyzing mucosal vascular patterns and “pillow sign” elasticity in real-time, potentially reducing the need for minimally invasive procedures. Additionally, the integration of Computer-Aided Diagnosis (CADx) is anticipated to reduce the “miss rate” of submucosal lesions during routine endoscopies.
3. Robotic and endoscopic cooperative surgery (RECS). Even though endoscopic and laparoscopic surgery are currently the gold standard for complicated cases, there is a possibility that RECS will gain popularity as robotic platforms provide improved 3D visualization and “wristed” dexterity, allowing for more precise full-thickness resections in difficult regions like the gastroesophageal junction.
4. Non-invasive targeted therapies. Subcutaneous lipomas have been effectively eliminated in recent years using non-invasive methods such as targeted injectables [43] and high-intensity focused ultrasound (HIFU) [44]. In the years to come, it is expected that these tools will be further investigated for the treatment of gastric lipomas without disrupting the stomach mucosa and without any requirement for a knife whatsoever.
5. The “gut-lipoma” microbiome connection. The gut microbiome (GM) and the formation of lipomas may be causally related, according to a recent line of research known as the microbiome-lipoma axis [45]. Future studies could examine if altering the gut flora can stop giant lipomas from growing or recurring.
Strengths and limitations
Strengths. This scoping review has a number of key strengths. First, it offers a thorough and current mapping of the clinical context of gastric lipoma over the past ten years, emphasizing a notable technical trend toward robotic and minimally invasive surgery. Second, a transparent and reproducible search approach was ensured by the review’s strict adherence to PRISMA-ScR (Extension for Scoping Reviews) principles. Lastly, a clinical observation about the threshold for “giant” stomach lipomas that was previously poorly defined in the literature was made attempted by the descriptive mapping.
Limitations. Several limitations must be acknowledged:
• Search constraint. After identification, the full text of the included articles were derived from the Saudi Digital Library, ResearchGate, Google Scholar and Open Access repositories. Consequently, some subscription-based articles may have been overlooked, potentially introducing a database bias.
• Level of evidence. There is an intrinsic flaw in any review that relies on case reports since they provide less data than randomized controlled trials. Rather than being a meta-analysis of management effectiveness, these findings should be seen as a map of documented cases.
• Publication bias. A critical limitation of this review is the inherent publication bias associated with case-report literature. The reliance on published cases likely results in an overestimation of symptomatic and complicated presentations, such as “giant” lipomas and severe gastrointestinal hemorrhage. An overestimation of symptomatic and complex presentations, like “giant” lipomas and severe gastrointestinal bleeding, is probably caused by the reliance on published cases. The large percentage of symptomatic cases found in this cohort (85.7%) may not accurately reflect the natural history of the disease in the general population since asymptomatic or minor incidentally identified lipomas are less likely to be reported. Therefore, rather than being a general diagnostic rule, the discovery that all lesions larger than 4 cm were symptomatic should be considered a clinical observation within a high-acuity subset of patients. This bias restricts how broadly the findings may be applied and emphasizes the necessity of population-based screening data to offer a more impartial clinical viewpoint.
• Follow-up data. A significant limitation identified in the mapped literature is the lack of longitudinal data; only a small percentage of cases provided follow-up for more than a year, which restricts our understanding of long-term recurrence rates.
Conclusion
This review provides a comprehensive map of the clinical landscape of gastric lipoma (GL) over the past decade. The findings confirm that while GL remains a rare clinical entity, it predominantly affects males in their sixth decade of life and most frequently originates in the gastric antrum. A critical clinical threshold was identified at 4 cm; lesions exceeding this size (giant GL) are almost universally symptomatic in the reported literature.
While a notable “decadal shift” toward minimally invasive techniques including laparoscopic (20.0%), robotic (5.7%), and advanced endoscopic resections (17.1%) ‒ is evident, conclusions regarding long-term safety and recurrence remain speculative. A significant knowledge gap exists, as fewer than 20% of cases reported longitudinal follow-up over one year, and nearly 55% provided no follow-up data at all. Consequently, the reported high success rate must be interpreted with caution due to inherent publication bias and the lack of robust surveillance protocols in the current literature. Future efforts must prioritize the establishment of multi-institutional registries to capture standardized, long-term outcome data and further define the role of parenchyma-sparing interventions.
Author contributions
Sajad Ahmad Salati ‒ study design, data collection, statistical analysis, manuscript preparation, literature search.
Mohammad Alfehaid ‒ data collection, statistical analysis, manuscript preparation, literature search.
Both the authors have approved the final manuscript.
Conflicts of interest
There is no conflict of interest.
Funding
This study has received no external funding.
Ethical approval
The scoping review analyzed the previously published and ethically approved case reports and hence no new ethical approval was required.
References
1. Cappell MS, Stevens CE, Amin M. Systematic review of giant gastric lipomas reported since 1980 and report of two new cases in a review of 117 110 esophagogastroduodenoscopies. World J Gastroenterol 2017; 23(30): 5619‒5633. DOI: 10.3748/wjg.v23.i30.5619.
2. Cherif M, Mesbahi M, Khedhiri N, Benzarti Y, Maamer AB. Gastric lipoma: An unusual cause of the upper gastrointestinal bleeding. Int J Surg Case Rep 2024; 119: 109684. DOI: 10.1016/j.ijscr.2024.109684.
3. Kumar S, Harisankar AG, Singh R, Kumar A, Kumar B, Mandal M. Lipoma of the gastrointestinal tract: A tertiary care centre experience. Ann R Coll Surg Engl 2024; 106(5): 401‒406. DOI: 10.1308/rcsann.2023.0063.
4. Wang S, Yang H, Jiang N, Jin S. Endoscopic resection of a giant broad-based gastric lipoma in an adolescent: A case report and literature review. BMC Pediatr 2025; 25(1): 388. DOI: 10.1186/s12887-025-05736-z.
5. Nasa M, Choksey A, Phadke A, Sawant P. Gastric lipoma: An unusual cause of dyspeptic symptoms. BMJ Case Rep 2016; 2016: bcr2016215297. DOI: 10.1136/bcr-2016-215297.
6. Al Shammari JO, Al-Shadidi N, Abdulsalam AJ, Al-Daihani AE. Gastric lipoma excision during a laproscopic sleeve gastrecomy: A case report. Int J Surg Case Rep 2016; 24: 128‒130. DOI: 10.1016/j.ijscr.2016.05.040.
7. Aoyama S, Ami K, Fukuda A, Imai K, Chong JM, Ando M. Gastric lipomatosis treated by total gastrectomy: A case report. Surg Case Rep 2017; 3(1): 126. DOI: 10.1186/s40792-017-0404-1.
8. Ichinose M, Hikichi T, Kanno Y, Gunji N, Fujita M, Kuroda M, Terashima K, Sato Y, Kawana S, Hashimoto Y, Ohira H, Miyata M. A case of gastric lipoma resected by endoscopic submucosa dissection with difficulty in preoperative diagnosis. Fukushima J Med Sci 2017; 63(3): 160‒164. DOI: 10.5387/fms.2016-19.
9. Termos S, Reslan O, Alqabandi O, AlDuwaisan A, Al-Subaie S, Alyatama K, Alali M, AlSaleh A. Giant gastric lipoma presenting as GI bleed: Enucleation or resection? Int J Surg Case Rep 2017; 41: 39‒42. DOI: 10.1016/j.ijscr.2017.10.004.
10. Amundson JR, Straus D, Azab B, Liu S, Garcia Buitrago MT, Yakoub D. Giant symptomatic gastric lipoma: A case report and literature review. Int J Surg Case Rep 2018; 51: 313‒317. DOI: 10.1016/j.ijscr.2018.08.061.
11. Krishnaraj B, Dhanapal B, Shankar G, Sistla SC, Galidevara I, Suresh A. Gastric lipoma: A rare cause of haematemesis. Ann R Coll Surg Engl 2018; 100(3): e41‒e43. DOI: 10.1308/rcsann.2017.0209.
12. Abdulrahman ME, Aji A, Alsabek MB. Incidental giant obstructed pedunculated gastric lipoma during gastrostomy: A case report. Int J Surg Case Rep 2018; 53: 433‒435. DOI: 10.1016/j.ijscr.2018.11.052.
13. Ingason AB, Theodors A, Agustsson AS, Arnarson A. Giant gastric lipoma successfully removed by endoscopic submucosal dissection: Case report and systematic review. Scand J Gastroenterol 2018; 53(8): 1018‒1024. DOI: 10.1080/00365521.2018.1495259.
14. Sharayah A, Unnikrishnan DC, Perumangote Vasudevan AA, Hajjaj N, Raj R, Belitsis K. A rare case of gastric lipoma presenting with gastric outlet obstruction treated endoscopically. Case Rep Gastrointest Med 2019; 2019: 5749830. DOI: 10.1155/2019/5749830.
15. Agafonoff S, Pitt T, Max J, Udelhofen S, Braverman TS, Lenobel RS. Simultaneous resection of a gastric submucosal lipoma in the setting of bariatric surgery: A case report and review of current literature. Int J Surg Case Rep 2019; 60: 216‒220. DOI: 10.1016/j.ijscr.2019.06.031.
16. Mir AS, Kesar V, Sageer M, Grider D, Chitnavis V. Bleeding gastric lipoma resected by endoscopic submucosal dissection. Cureus 2020; 12(6): e8909. DOI: 10.7759/cureus.8909.
17. Sabbah M, Nakhli A, Helal I, Bellil N, Ouakaa A, Gargouri D. Gastrointestinal bleeding as an initial manifestation of gastric lipoma: Case report and review of the literature. Clin Case Rep 2020; 8(10): 1988‒1992. DOI: 10.1002/ccr3.3050.
18. Kumar S, Kumar A, Dayal M, Prakash V. Gastric lipoma: A rare cause of massive haematemesis. Ann R Coll Surg Engl 2021; 103(6): e196‒e198. DOI: 10.1308/rcsann.2020.7094.
19. Lalanda R, Suárez González R. Enucleation of ulcerated gastric lipoma after massive melaena. BMJ Case Rep 2021; 14(8): e244686. DOI: 10.1136/bcr-2021-244686.
20. Solis M, Rivera AS, Shakhatreh M, Rapoport G, Albustamy A, Zamir A. Gastric lipoma in a patient with symptomatic GERD. Am J Gastroenterol 2021; 116: pS1515. DOI: 10.14309/01.ajg.0000789192.21305.c8.
21. Parreira R, Rama T, Eloi T, Carneiro V, Leite MI. Enucleation of a giant symptomatic gastric lipoma, a safe surgical approach. J Surg Case Rep 2021; 2021(3): rjab087. DOI: 10.1093/jscr/rjab087.
22. Rezaii S, Enshaii A, Zahedi A, Amestejani M, Herik Dizaji M. Gastrointestinal bleeding due to gastrointestinal lipoma: A case report. Caspian J Intern Med 2021; 12(4): 622‒625. DOI: 10.22088/cjim.12.4.622.
23. Marques P, Santos A, Germano A. Ulcerated gastric lipoma presenting with gastrointestinal bleeding and hypovolemic shock. J Belg Soc Radiol 2022; 106(1): 2. DOI: 10.5334/jbsr.2700.
24. Nabi Z, Ramchandani M, Darisetty S, Reddy DN. Endoscopic resection of a large submucosal tumor causing intermittent gastric outlet obstruction using a novel radiofrequency enabled device. Dig Dis 2022; 40(1): 119‒122. DOI: 10.1159/000515855.
25. Hussein Al-Janabi MA, Mohammad JG, Mohsen AY, Alabbas Z, Rasheed O, Kannan S, Daoud AK. Gastric lipoma in the pyloric antrum: A rare case report. Ann Med Surg (Lond) 2023; 85(10): 5110‒5112. DOI: 10.1097/MS9.0000000000001131.
26. Martins R, Morais H. Giant gastric lipoma: A case report and literature review. Rev Port Cir 2023; 56: 1016. DOI: 10.34635/rpc.1016.
27. Al-Anbagi U, Aljuboori ZA, Nashwan AJ, Salehi A. A case report on gastric lipoma: An unusual etiology of gastrointestinal bleeding. Cureus 2024; 16(12): e76699. DOI: 10.7759/cureus.76699.
28. Chaouch MA, Taieb AH, Maaref M, Baccari L, Saad J, Noomen F. Laparoscopic resection of a gastric lipoma following massive upper gastrointestinal bleeding: A case report. Int J Surg Case Rep 2024; 120: 109876. DOI: 10.1016/j.ijscr.2024.109876.
29. Jarrett SA, Tito S, Chan M, Jarrett DE, Lo KB, DePalma R. Gastric lipomas: A case series and review of the literature. Case Rep Gastroenterol 2024; 18(1): 14‒20. DOI: 10.1159/000534973.
30. Qadir NA, Stachler L, Rai O, Suarez LSK, Ribeiro B. Heavy on the belly: A curious case of a large ulcerated gastric lipoma-inducing syncope. Am J Gastroenterol 2024; 119(10S): S3221‒S3222. DOI: 10.14309/01.ajg.0001049908.40259.41.
31. Rasmussen IR, Grossjohann H, Kristensen TS, Penninga L. Gastric lipoma presenting with gastrointestinal bleeding. BMJ Case Rep 2024; 17(2): e259345. DOI: 10.1136/bcr-2023-259345.
32. Setake M, Shiroma M, Tomiyama M, Tasato Y, Mabuchi H, Kinjo Y, Miyazato M, Nakachi N, Shimajiri H, Tomiyama R, Chinen Y, Hokama A. A gastric lipoma that grew in size in seven years presenting bleeding. Chonnam Med J 2024; 60(1): 89‒90. DOI: 10.4068/cmj.2024.60.1.89.
33. Thomas T, Wilson S, James E. Exploring the link between gastric lipoma and glycemic variability: A case report. IJFMR 2024; 6(6): 1‒3. DOI: 10.36948/ijfmr.2024.v06i06.31579.
34. Joshi A, Kumar R, Shah M, Mui R, Hiatt TK. Unusual presentation of acute gastrointestinal bleeding in gastric lipoma and concomitant Helicobacter pylori infection: A case report. Clin Case Rep 2025; 13(3): e70311. DOI: 10.1002/ccr3.70311.
35. Dargan P, Sodhi P, Jain BK. Bleeding gastric lipoma: Case report and review of the literature. Trop Gastroenterol 2003; 24(4): 213‒214.
36. Rao C, Rana SS, Lal A, Kumar M, Behera A, Dahiya D, Joshi K, Bhasin DK. Large gastric lipoma presenting with GI bleeding. Gastrointest Endosc 2013; 77: 512‒513. DOI: 10.1016/J.GIE.2012.10.022.
37. Ramdass MJ, Mathur S, Seetahal-Maraj P, Barrow S. Gastric lipoma presenting with massive upper gastrointestinal bleeding. Case Rep Emerg Med 2013; 2013: 506101. DOI: 10.1155/2013/506101.
38. Chen Y, Andrews CN. Luminal lipoma: The “pot-of-gold” sign. Gastrointest Endosc 2014; 79(1): 167. DOI: 10.1016/j.gie.2013.08.036.
39. Taylor AJ, Stewart ET, Dodds WJ. Gastrointestinal lipomas: A radiologic and pathologic review. Am J Roentgenol 1990; 155(6): 1205‒1210. DOI: 10.2214/ajr.155.6.2122666.
40. Thompson WM, Kende AI, Levy AD. Imaging characteristics of gastric lipomas in 16 adult and pediatric patients. Am J Roentgenol 2003; 181(4): 981‒985. DOI: 10.2214/ajr.181.4.1810981.
41. Shimada S, Ishizawa T, Ishizawa K, Matsumura T, Hasegawa T, Hirose T. The value of MDM2 and CDK4 amplification levels using real-time polymerase chain reaction for the differential diagnosis of liposarcomas and their histologic mimickers. Hum Pathol 2006; 37: 1123‒1129. DOI: 10.1016/j.humpath.2006.04.010.
42. Boltze C, Schneider-Stock R, Jäger V, Roessner A. Distinction between lipoma and liposarcoma by MDM2 alterations: A case report of simultaneously occurring tumors and review of the literature. Pathol Res Pract 2001; 197: 563‒568. DOI: 10.1078/0344-0338-00128.
43. Santiago-Vázquez M, Michelen-Gómez EA, Carrasquillo-Bonilla D, Carrasquillo OY, Cruz A. Intralesional deoxycholic acid: A potential therapeutic alternative for the treatment of lipomas arising in the face. JAAD Case Rep 2021; 13: 112‒114. DOI: 10.1016/j.jdcr.2021.04.037.
44. Shemer A, Brawer S, Amichi B, Azhari H. Noninvasive lipoma size reduction using high-intensity focused ultrasound. Dermatol Surg 2013; 39(10): 1446‒1451. DOI: 10.1111/dsu.12269.
45. Li Y, Chen J, Yao H, Xu X, Zheng X, Wang Y, Wang W. Gut Microbiota’s role in lipoma development: Evidence from mendelian randomization. Front Genet 2024; 15: 1430671. DOI: 10.3389/fgene.2024.1430671.