Psichologija ISSN 1392-0359 eISSN 2345-0061
2025, vol. 73, pp. 95–111 DOI: https://doi.org/10.15388/Psichol.2025.73.7
Does Successful Aging Moderate the Link between Chronic Pain and Depressive Symptoms?
Kamilė Naujalytė
Vilnius University, Faculty of Philosophy, Institute of Psychology
kamile.naujalyte@alumni.vu.lt
https://orcid.org/0009-0001-1742-1018
https://ror.org/03nadee84
Rūta Sargautytė
Vilnius University, Faculty of Philosophy, Institute of Psychology
ruta.sargautyte@fsf.vu.lt
https://orcid.org/0000-0002-4555-4889
https://ror.org/03nadee84
Abstract. This study investigated whether the relationship between chronic pain and depression in older adults can be moderated by successful aging, based on the SOC theory (Baltes & Baltes, 1990). Its participants included 106 individuals aged 65 to 93 (M = 72.12, SD = 6.39), of whom, 89.6% were female and 10.4% male. Chronic pain was assessed by using the Pain Intensity, Enjoyment of Life and General Activity Scale (Krebs et al., 2009), depression was measured by using the Geriatric Depression Scale (Sheikh & Yesavage, 1986), and successful aging was assessed by using the Selection, Optimization, and Compensation Questionnaire (Freund & Baltes, 2002; Segura-Camacho et al., 2018). A cross-sectional correlational design was applied by using correlational and moderation regression analyses. The results showed a positive association between chronic pain and depression. Notably, the compensation strategy moderated this relationship: if using the compensation strategy less frequently, greater chronic pain predicted higher depression, while using compensation strategy more frequently the relationship between chronic pain and depression weakened. These findings highlight the role of compensation in moderating the association between depression and chronic pain in older adults. Despite its limitations, the study contributes to a deeper understanding of opportunities for improving psychological support for older adults experiencing chronic pain.
Keywords: chronic pain, depression, successful aging, SOC, compensation.
Ar sėkmingas senėjimas moderuoja ryšį tarp lėtinio skausmo ir depresiškumo?
Santrauka. Šiame tyrime buvo nagrinėjama, ar ryšį tarp vyresnio amžiaus žmonių lėtinio skausmo ir depresiškumo gali moderuoti sėkmingas senėjimas, aiškinamas SOC teorija (Baltes & Baltes, 1990). Tyrime dalyvavo 106 asmenys, kurių amžius svyravo nuo 65 iki 93 metų (M = 72,12, SD = 6,39); 89,6 proc. sudarė moterys, 10,4 proc. – vyrai. Lėtiniam skausmui įvertinti buvo naudojamas Skausmo intensyvumo, mėgavimosi gyvenimu ir bendros veiklos klausimynas (Krebs et al., 2009), depresiškumui – Geriatrinė depresijos skalė, trumpoji versija (Sheikh & Yesavage, 1986), sėkmingam senėjimui – Selekcijos, optimizacijos ir kompensacijos klausimynas, trumpoji versija (Freund & Baltes, 2002; Segura-Camacho et al., 2018). Atliktas skerspjūvio koreliacinis tyrimas, taikyta koreliacinė bei moderacinė regresinė analizės. Tyrimo rezultatai atskleidė teigiamą ryšį tarp lėtinio skausmo ir depresijos. Gauta, kad kompensacijos strategija moderavo šį ryšį: rečiau naudojantis kompensacijos strategija, didesnis lėtinis skausmas nuspėjo didesnį depresiškumą, o naudojantis kompensacija dažniau – ryšys tarp lėtinio skausmo ir depresiškumo susilpnėjo. Šie rezultatai pabrėžia kompensacijos strategijos vaidmenį silpnesniam ryšiui tarp depresiškumo ir lėtinio skausmo vyresniame amžiuje. Nepaisant tam tikrų trūkumų, tyrimas prisideda prie gilesnio supratimo apie psichologinės pagalbos gerinimo galimybes vyresnio amžiaus žmonėms, patiriantiems lėtinį skausmą.
Pagrindiniai žodžiai: lėtinis skausmas, depresija, sėkmingas senėjimas, SOC, kompensacija.
Received: 2025-04-01. Accepted: 2025-07-16.
Copyright © 2025 Kamilė Naujalytė, Rūta Sargautytė. Published by Vilnius University Press. This is an Open Access article distributed under the terms of the Creative Commons Attribution Licence (CC BY), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction
In recent decades, the proportion of older adults has grown significantly in Lithuania as well as worldwide. From 2013 to 2023, Lithuania’s population aged 65 and older increased from 18.2% to 20%, with the median age rising by 2 years (Eurostat, 2024; Oficialiosios statistikos portalas, 2024). The World Health Organization projects that, by 2030, one in six people globally will be 60 years or older, doubling by 2050 (World Health Organization, 2024).
Aging introduces various physical, psychological, cognitive, social, and financial challenges. This life stage often involves losses, including those of family members, friends, health, employment, and social roles (Siren & Hakamies-Blomqvist, 2009; Nikitin & Freund, 2019). Such experiences can lead to suffering, grief, and a heightened depression risk (Scur et al., 2021). Therefore, research is needed to explore older adults’ abilities to adapt and cope with the challenges of aging.
Chronic pain and depression
One of the most prevalent health-related issues associated with aging is chronic pain. The International Classification of Diseases (ICD-11) defines it as pain lasting more than 3 months (World Health Organization, 2019). Chronic pain involves sensory, physical, and emotional aspects (Krebs et al., 2009), with its likelihood increasing with age (Domenichiello & Ramsden, 2019). In 2021, 30% to 34.3% of Americans aged 65 and older reported chronic pain, while an additional 10.4% to 14.3% experienced severe pain limiting daily activities. In comparison, the prevalence rates among adults aged 25 to 44 years were 13.7% and 3.5%, respectively (Rikard et al., 2023).
Chronic pain heightens the risk of depression (Agüera-Ortiz et al., 2015; Zis et al., 2017; Nguyen et al., 2021) and suicide (Santos et al., 2020). The relationship between chronic pain and depression can be bidirectional, with 55.2% of individuals with depression reporting chronic pain (Liu et al., 2021) and 56.5% to 70% of those with chronic pain experiencing depressive symptoms (Agüera-Ortiz et al., 2013; Nguyen et al., 2021). A higher pain intensity often correlates with more severe depression (Agüera-Ortiz et al., 2013). This phenomenon is sometimes referred to as Chronic Pain-Induced Depression (Sheng et al., 2017; Meda et al., 2022).
From a cognitive perspective, Zis et al. (2017) describe the relationship as a self-reinforcing cycle. Pain triggers negative emotions like anxiety and sadness, leading to heightened pain perception and avoidance behaviors, which exacerbate depressive symptoms. Therefore, it is crucial to understand the factors mitigating these effects. Evidence suggests that successful aging strategies, such as selection, optimization, and compensation, may play a significant role in this context (Alonso-Fernández et al., 2016; Zhang & Radhakrishnan, 2018).
Successful aging
Models of successful aging are divided into two categories: (1) outcome-based models, which define successful aging by observable results in later life, and (2) process-based models, viewing it as a lifelong adaptive process balancing losses and gains. Outcome-based models face criticism for their unrealistic criteria, such as the absence of serious illness, thereby disregarding the abilities and accomplishments of older adults. Process-based models prioritize adaptability, recognizing that even those facing challenges can achieve successful aging through adaptive processes (Villar, 2012).
One of the most influential process-based models is the Selection, Optimization, and Compensation (SOC) theory, proposed by Baltes and Baltes (1990). Despite being established over 30 years ago, the SOC theory remains relevant and is mainly used in contemporary research on older adults’ work capacity and adaptability (Riedel et al., 2015; Weber et al., 2018; Meng et al., 2022). SOC involves three strategies: selection, optimization, and compensation. Selection involves narrowing activities to prioritize those that are aligned with the individual goals, capabilities, and environmental demands. Meanwhile, optimization focuses on maximizing performance in prioritized activities by dedicating resources such as time and effort. Finally, compensation entails adopting new tools, skills, or external support when the existing abilities decline. How these adaptation components are realized depends on the specific personal and societal circumstances individuals face as they age (Baltes & Baltes, 1990; Baltes et al., 1999). Ultimately, successful aging is an ongoing adaptive process, emphasizing that older adults can actively achieve well-being (Baltes & Carstensen, 1996; Baltes & Baltes, 1990).
Successful aging, chronic pain, and depression
Research suggests that the use of successful aging strategies, specifically, Selection, Optimization, and Compensation (SOC), in the context of chronic pain, may be associated with reduced depression symptoms, though supporting sources are limited. Alonso-Fernández et al. (2016) found that Acceptance and Commitment Therapy (ACT), combined with SOC training, improved emotional well-being, pain acceptance, and functional capacity in elderly individuals with chronic pain. It also reduced pain catastrophizing, depression, and anxiety compared to a control group with minimal assistance. Zhang and Radhakrishnan (2018) supported this, by showing that the use of SOC strategies was associated with lower levels of depressive symptoms, greater pain acceptance, and more positive views on aging. Additionally, SOC strategies used in pain interventions were linked to decreased medication use and greater life satisfaction.
However, Warner et al. (2019) found no significant association between SOC strategies and the relationship between chronic health problems and depression in elderly women, possibly because only some participants experienced chronic pain, and adaptive strategies were not analyzed separately. The availability of resources also affects the use of SOC strategies, with individuals often focusing on selection due to financial or social limitations (Janke et al., 2009). This explains why the significance of SOC strategies may vary.
In summary, while successful aging may relate to the way chronic pain and depression are connected, it remains insufficiently explored, worldwide as well as specifically in Lithuania. This study aims to investigate whether successful aging, measured by the use of SOC strategies, moderates the relationship between chronic pain and depressive symptoms in older adults. Two hypotheses were proposed:
H1: Higher levels of chronic pain are associated with greater depressive symptoms.
H2: Chronic pain will be a weaker predictor of depressive symptoms in individuals with higher levels of successful aging and more frequent use of SOC strategies.
Methodology
Participants and procedure
The survey was conducted from November 2023 to January 2024 in Lithuania, with the questionnaire provided in Lithuanian. Two scales (PEG and SOC) were professionally translated into Lithuanian and piloted with a small group of older adults (n = 3) to assess their clarity. Minor wording adjustments were made based on the feedback. It was a cross-sectional correlational study targeting individuals aged 65 and older experiencing chronic pain. The participants were selected through convenience sampling from polyclinics, pharmacies, and public organizations. The responses were collected in both paper and online formats. Thirteen questionnaires were excluded due to improper completion, leaving 106 participants in total. Since the target group is vulnerable to psychological difficulties, psychological help guidelines were included with the survey.
The participants’ ages ranged from 65 to 93 years, with an average age of 72.12 years (SD = 6.39). Sociodemographic characteristics including gender, education, marital status, and employment status are presented in Table 1.
Table 1
Sociodemographic characteristics of the study participants (N = 106)
|
n |
% |
|
|---|---|---|
|
Gender |
||
|
Female |
95 |
89.6 |
|
Male |
11 |
10.4 |
|
Education |
||
|
Primary, secondary, or special secondary |
24 |
22.9 |
|
Higher vocational or college |
30 |
28.6 |
|
Higher university |
51 |
48.6 |
|
Marital status |
||
|
Without a partner or widowed |
56 |
52.8 |
|
Having a partner or spouse |
50 |
47.2 |
|
Employment status |
||
|
Not working or retired |
88 |
83 |
|
Employed |
18 |
17 |
Note. n = number of participants; % = percentage.
Variables and their measures
The first part of the questionnaire included sociodemographic questions (gender, age, education, marital status, and employment) along with two screening questions to confirm the presence of chronic pain (“Chronic pain refers to body pain that lasts or recurs for 3 months or longer. Do you experience chronic pain?”, “If you experience chronic pain, how long have you been living with it?”).
Pain Intensity, Enjoyment in Life and General Activity Scale (PEG) assesses chronic pain through three dimensions: pain intensity, activity interference, and life satisfaction interference (“What number best describes how, during the past week, pain has interfered with your general activity?”) (Krebs et al., 2009). It consists of three items in total. The participants rate the impact of pain over the past week on a 0–10 Likert scale, with higher scores indicating more chronic pain. The original version is reliable and valid (Krebs et al., 2009). The PEG questionnaire has also been translated and validated in Spanish (Kapos et al., 2023). Permission to translate the questionnaire into Lithuanian and use it in this study was obtained from the authors. The Lithuanian version showed a reliability of α = 0.84 in this study. The conducted Confirmatory Factor Analysis (CFA) confirmed good validity (χ² = 0, df = 0, p < 0.001; RMSEA = 0.0, p < 0.001; CFI = 1.0, TLI = 1.0; factor loadings: 0.61, 0.98, 0.84; p < 0.001). Full CFA for chronic pain factors is presented in Annex A (Figure A).
The Geriatric Depression Scale (GDS-15) short version, used to assess depression in older adults (Sheikh & Yesavage, 1986), consists of 15 self-administered questions. Examples include: “Are you basically satisfied with your life?” and “Do you prefer to stay at home, rather than going out and doing new things?”. The offered response options are ‘Yes’ or ‘No’, with five questions reversed. The score is the sum of ‘Yes’ responses, where each ‘yes’ answer equals ‘1’. A higher score indicates greater depression. The reliability and validity of the short version have been found to be adequate (Friedman et al., 2005). The GDS has been translated into multiple languages, including Lithuanian (Alseikienė, 1999), and showed good reliability (α = 0.89) for the long version (Deksnytė et al., 2012). The Lithuanian version of the scale is available for public use at www.stanford.edu/~yesavage/GDS.html. In this study, the reliability of the Lithuanian version was α = 0.86. The conducted CFA (χ² = 118.61, df = 88, p = 0.017; RMSEA = 0.06, p = 0.315; CFI = 0.92, TLI = 0.90) revealed factor loadings between 0.20 and 0.71, with 14 out of 15 being significant (p < 0.05), although four questions had loadings below 0.4, and one was marginally non-significant (p = 0.055). Full CFA for depression factors is presented in Annex B (Figure B).
The Selection, Optimization, and Compensation Questionnaire (SOC-12) assesses successful aging through the concepts of selection, optimization, and compensation. Initially developed in German and later translated into English (Baltes et al., 1999), it includes four subscales: elective selection, loss-based selection (which are combined into a general selection subscale in this study), optimization, and compensation. The questionnaire has been translated into languages such as Chinese (Chou & Chi, 2001), Swedish (Viglund et al., 2013), Japanese (Okabayashi, 2014), Spanish (Segura-Camacho et al., 2018), and Polish (Zając-Lamparska, 2021), with adequate psychometric characteristics for measuring SOC strategies. In the Spanish version, participants rate statements on a Likert scale from 1 (‘never’) to 5 (‘always’), to reflect the frequency of use of the SOC strategies (Segura-Camacho et al., 2018). This version is reliable and valid (Geldhof et al., 2015). The Spanish version, translated into Lithuanian, was used in this study with its authors’ permission.
See a few examples of items: Selection: “When I can’t do something important the way I did before, I look for a new goal”. Optimization: “I make every effort to achieve a given goal”. Compensation: “When something isn’t working as well as it used to, I ask others for help”. The reliability of the questionnaire was assessed with internal consistency: overall α = 0.86, Selection α = 0.81, Optimization α = 0.73, Compensation α = 0.50. The conducted CFA (χ² = 74.89, df = 50, p = 0.013; RMSEA = 0.07, p = 0.170; CFI = 0.93, TLI = 0.90) showed that factor loadings ranged from 0.55 to 0.81 (p < 0.001) for the Selection subscale, from 0.64 to 0.80 (p < 0.001) for the Optimization subscale, and two factors had loadings of 0.63 (p < 0.001) for the Compensation subscale, with one factor at 0.25 (p < 0.05). Full CFA for successful aging factors is presented in Annex C (Figure C). As shown in Figure C, two standardized correlations between latent factors exceed a value of 1, thus suggesting the limited validity of the scale. Although merging the subscales could address this issue, we chose to retain the original factor structure so that to remain consistent with the validated version of the scale.
Statistical analysis
Statistical analysis was performed by using IBM SPSS Statistics 29.0 and Structural Equation Modeling (SEM) with Mplus. Descriptive statistics (means, standard deviations) were calculated in SPSS, and the scale reliability was assessed by using internal consistency (α). The scale variables were created by using mean scores. The normality of data was tested by using the Kolmogorov-Smirnov test, Skewness, Histogram, Normal Q-Q plot, and Detrended Q-Q plot. Chronic Pain, Successful Aging, Selection, and Compensation were normally distributed, while Depression and Optimization were not. Non-normally distributed variables were transformed by using square root transformation to meet the assumptions of parametric tests. Parametric tests were applied to normally distributed and transformed variables. Pearson correlation assessed the relationships between the variables. Moderation regression analysis was conducted by using Hayes’ SPSS Process Macro 4.2 (Model 1). In Mplus, Confirmatory Factor Analysis (CFA) was used to assess the scale validity, evaluated by four model fit criteria: Chi-square (χ²), RMSEA, CFI, and TLI. The CFA for the PEG scale was conducted by using the Maximum Likelihood (ML) estimator, as the data were normally distributed. For the GDS and SOC scales, Maximum Likelihood with Robust standard errors (MLR) was used due to the non-normal distribution of the data. The results were considered statistically significant when p < 0.05.
Results
The means and standard deviations of the study constructs are presented in Table 2.
Table 2
Means and standard deviations of the study constructs in the study sample (N = 106)
|
Scale |
M |
SD |
|---|---|---|
|
Chronic pain |
5.79 |
2.22 |
|
Depression |
5.58 |
3.92 |
|
Successful aging (SOC) |
3.77 |
0.70 |
|
Selection |
3.67 |
0.79 |
|
Optimization |
2.01 |
0.20 |
|
Compensation |
3.64 |
0.80 |
Note. M = mean; SD = standard deviation.
The first objective was to determine if chronic pain in older adults is associated with depression. The relevant hypothesis (H1) proposed that greater chronic pain is linked to greater depression. Pearson correlation analysis revealed a weak positive and statistically significant correlation between chronic pain and depression, r = 0.26, N = 106, p = 0.007, confirming that greater chronic pain is associated with greater depression. Thus, hypothesis H1 was confirmed.
The second objective was to examine if successful aging (SOC) moderates the relationship between chronic pain and depression in older adults. Hypothesis H2 suggested that chronic pain would be a weaker predictor of depression in those with higher successful aging indicators and more frequent use of its strategies. A moderation analysis was used to test this hypothesis, as illustrated in Figure 1.
Figure 1
Theoretical model of moderation
![[Figure 1 presents a theoretical moderation model illustrating the proposed relationships between chronic pain, successful aging (SOC), and depression. In this model, chronic pain is depicted as an independent variable influencing depression as the dependent variable. Successful aging, represented by the Selection, Optimization, and Compensation (SOC) model, acts as a moderator. The direct path from chronic pain to depression suggests an association between pain and depressive symptoms. The additional path from successful aging to the relationship between chronic pain and depression suggests that SOC may moderate the association between chronic pain and depression. This conceptual framework serves as the basis for investigating the moderating role of successful aging strategies in the relationship between chronic pain and mental health outcomes.]](https://www.zurnalai.vu.lt/psichologija/article/download/40090/version/36232/40522/124391/theor3.png)
The study data were divided into two groups based on successful aging levels: high successful aging (equal to or above the sample average, n = 52), and low successful aging (below the sample average, n = 54). Successful aging was treated as a dichotomous variable (high or low). Chronic Pain was the independent variable, Depression was the dependent variable, and Successful Aging (SOC) served as the moderator. The analysis showed a good model fit (F(3, 102) = 4.44, p = 0.006, R² = 0.12). The interaction between Chronic Pain and Successful Aging in the model was statistically non-significant (B = -0.02, p = 0.427), suggesting that Successful Aging does not moderate the relationship between Chronic Pain and Depression. In this sample, the ability to adapt to aging-related changes was not significantly associated with changes in the relationship between chronic pain and depression.
The moderation analysis was repeated for each adaptive strategy to see if the results were specific to each strategy. The participants were divided into two groups based on the use of the selection strategy: those using it more frequently (equal to or above the sample average, n = 50) and those using it less frequently (below the sample average, n = 56). Selection was treated as a dichotomous variable (high versus low use). Chronic Pain was the independent variable, Depression served as the dependent variable, and Selection was the moderator. The analysis showed a good model fit (F(3, 102) = 5.80, p = 0.001, R² = 0.15). The interaction between Chronic Pain and Selection in the model was statistically non-significant (B = -0.01, p = 0.820), thereby indicating that Selection does not moderate the relationship between Chronic Pain and Depression. In this sample, the use of the selection strategy was not associated with changes in the link between chronic pain and depression.
Further, the role of the successful aging strategy of optimization in the relationship between chronic pain and depression was examined. The participants were divided into two groups based on their use of optimization: those who used it more frequently (equal to or above the sample mean, n = 52), and those who used it less frequently (below the mean, n = 54). Optimization was treated as a dichotomous variable (high or low use). Chronic Pain was the independent variable, Depression was used as the dependent variable, and Optimization was the moderator. The moderation analysis showed a good model fit (F(3, 102) = 4.90, p = 0.003, R² = 0.13). The interaction between Chronic Pain and Optimization was statistically non-significant (B = -0.01, p = 0.803), thereby indicating that Optimization does not moderate the relationship between Chronic Pain and Depression. In this sample, the use of the optimization strategy was not associated with changes in the link between chronic pain and depression.
The final step was to examine whether the compensation strategy moderates the relationship between chronic pain and depression. The participants were divided into two groups based on their frequency of compensation use: those who used it more frequently (equal to or above the mean, n = 64) and those who used it less frequently (below the mean, n = 42). Compensation was a dichotomous variable (high versus low use). Chronic Pain was the independent variable, Depression was treated as the dependent variable, and Compensation was the moderator. The moderation analysis showed good model fit (F(3, 102) = 4.90, p = 0.003, R² = 0.13). The interaction between Chronic Pain and Compensation in the model was statistically significant (B = -0.05, p = 0.036), thus indicating that compensation moderates the relationship between chronic pain and depression. The results are presented in Table 3.
Table 3
Moderation analysis results where the moderator in the relationship between chronic pain and depression is compensation
|
B |
se |
t(df) |
p |
|
|---|---|---|---|---|
|
Chronic pain |
0.07 |
0.02 |
2.78 (102) |
0.006 |
|
Compensation |
-0.02 |
0.02 |
-0.76 (102) |
0.447 |
|
Chronic pain and Compensation interaction |
-0.05 |
0.02 |
-2.12 (102) |
0.036 |
Note. B = unstandardized beta; se = standard error; t = t test statistic; df = degrees of freedom; p = probability value. Statistically significant results are highlighted in bold.
An interaction plot (Figure 2) was created to better understand how compensation moderates the relationship. The plot shows that, for those using compensation less frequently, greater chronic pain predicts higher depression. However, for those using compensation more frequently, depression levels remain stable. Thus, frequent use of compensation was associated with a weaker relationship between chronic pain and depression.
Simple linear regression was performed for the low and high compensation groups to assess whether the relationship between chronic pain and depression diminishes or ceases. In the low compensation group, the results were statistically significant (F = 10.95, p = 0.002; R² = 0.22, β = 0.46, p = 0.002), thus indicating that higher chronic pain predicts greater depression. In the high compensation group, the results were statistically non-significant (F = 0.73, p = 0.397; R² = 0.01, β = 0.11, p = 0.397), which means that chronic pain is not associated with depression for those using compensation more frequently. Therefore, the frequent use of compensation moderates this relationship by breaking it.
Figure 2
Interaction between chronic pain and compensation in predicting depression
![[This figure presents a line graph showing the relationship between chronic pain and depression, with compensation as a moderating variable. The x-axis represents chronic pain, with two levels: Low Chronic Pain on the left and High Chronic Pain on the right.
The y-axis represents depression, ranging from 0 to 1, with intermediate values labeled at 0.25, 0.5, and 0.75. A legend on the right distinguishes between the two compensation levels – low and high. Two lines depict the relationship:
The solid line represents Low Compensation (indicated by diamond markers). It shows an increasing trend, which means that as chronic pain increases, depression also increases. The dashed line represents High Compensation (indicated by circular markers). It shows a flatter trend, indicating that as chronic pain increases, depression remains relatively stable.]](https://www.zurnalai.vu.lt/psichologija/article/download/40090/version/36232/40522/124390/inter4.png)
In conclusion, hypothesis H2 was partially confirmed. Successful aging (SOC) did not moderate the chronic pain-depression relationship. Selection and optimization showed no significant association, but compensation did. When the compensation use was higher, the relationship between chronic pain and depression ceased. Thus, chronic pain is not linked to depression when compensation strategies are frequently used.
Discussion
This study explores the role of successful aging (SOC) and its strategies in the relationship between chronic pain and depression in older adults. The first step was to determine if chronic pain is linked to depression, and the analysis confirmed that higher chronic pain is associated with greater depression, thus supporting the research hypothesis. Similar findings have been reported in previous studies (Agüera-Ortiz et al., 2013; Bernfort et al., 2015; Zis et al., 2017; Santos et al., 2020; Nguyen et al., 2021).
The primary objective was to investigate whether successful aging (SOC) and its strategies could moderate this relationship. While some studies suggest that SOC plays a role in this connection (Alonso-Fernández et al., 2016; Zhang & Radhakrishnan, 2018), the hypothesis that chronic pain would be a weaker predictor of depressive symptoms in individuals with higher levels of successful aging was only partially supported. SOC did not moderate the relationship, nor did selection and optimization strategies. However, the compensation strategy moderated the relationship: for those who used compensation less frequently, greater chronic pain predicted greater depression, whereas, for frequent compensation users, the link between chronic pain and depression weakened. This suggests that compensation may act as a protective factor against depression in older adults with chronic pain.
Several studies highlight the distinct role of compensation among SOC strategies (Weber et al., 2018; Warner et al., 2019). For example, Warner et al. (2019) found that successful aging, as defined by the SOC model, was not significantly associated with changes in the relationship between chronic health problems (e.g., chronic diseases, pain, and physical disabilities) and depression in older women. Their analysis used a general measure of successful aging, without differentiating between individual strategies, which limited their ability to explore the topic in detail. However, they also tested the role of social support, which was significant and interpreted as a mechanism to reduce depression and loneliness. Social support is one of the key aspects of the compensation strategy (Freund & Baltes, 2002), suggesting that compensation plays a role in linking chronic diseases and depression, which is a finding consistent with the results of this study. In another study, Weber et al. (2018) examined SOC strategies for maintaining workability in older workers and found that only compensation showed a significant association with maintaining workability. They argued that compensatory measures effectively address age-related resource declines (Weber et al., 2018). Unlike selection and optimization, compensation allows individuals to maintain prior goals, while minimizing the impact of the aging process on aspirations (Baltes & Carstensen, 1996). In this study, compensation was found to significantly moderate the relationship between chronic pain and depression, possibly acting as a protective factor when chronic pain levels get higher.
The strength of the SOC model lies in its recognition of individuals’ ability to proactively adapt to aging changes, offering methods to cope with physical, psychological, and social changes, and encouraging behavioral adjustments (Freund & Baltes, 2002). The model aims to enhance self-efficacy – i.e., the belief in one’s ability to control motivation and behavior to achieve goals (Baltes & Carstensen, 1996). Individuals applying this model decide which goals to pursue, when to exert effort, and when to compromise.
A limitation of the SOC model is that older adults’ ability to optimize or compensate may be constrained by the available resources. Janke, Son, and Payne (2009) found that limited resources often lead individuals to focus on selection rather than other SOC processes that require more financial or social support. Therefore, the model should consider financial and social realities, especially in terms of compensation, which was key for emotional well-being in this study. The SOC model can complement interventions for older adults with chronic pain, helping maintain emotional well-being and activity engagement (Riedel et al., 2015). This study suggests that psychological support for older adults with chronic pain could focus on helping them use compensatory strategies to sustain life goals. Insufficient compensation use can predict greater emotional distress, so SOC diagnostics could help identify individuals for pain management programs. Additionally, there are efforts to integrate the SOC model with contemporary therapeutic approaches like the Acceptance and Commitment Therapy (Moeller & O’Brien, 2024).
Speaking of financial and social realities, the socioeconomic status of the aging group in Lithuania is reflected in recommendations to health, social, employment, education, and science policymakers, based on data from the 7th wave of the Survey of Health, Aging, and Retirement in Europe (SHARE) (Kairys et al., 2021). Lithuania’s results, based on 2,014 interviews with people aged 50 and older, are worse than the EU average in assessing the population’s well-being and its contributing factors. In total, 62.7% of Lithuanian respondents reported social activity below the average, and multimorbidity (having more than one chronic disease) not only complicates the treatment process and increases the need for healthcare services but also influences the frequency of mood or emotional disorders. In 2020, 36% of people aged 65 and older lived below the poverty line. While these factors may limit compensation strategies, other factors in providing healthcare and social services could also be significant. The SHARE survey data (Kairys et al., 2021) indicate that health literacy and understanding of the importance of preventive measures among Lithuanian residents aged 50 and older are insufficient, thus suggesting that the promotion of self-care could enhance self-reflection about health and ageing and foster the use of SOC strategies. Additionally, healthcare professionals, particularly primary care providers, should adopt a more proactive role in ensuring access to the necessary care (Kairys et al., 2021), thereby strengthening motivation for exploring inner resources or learning new self-management skills.
This study had several limitations. A cross-sectional design limits causal conclusions, and therefore the direction of relationships is based only on theoretical assumptions. The data were collected by using convenience sampling, and thus the findings cannot be generalized to all older adults in Lithuania. A large portion of the sample (89.6%) consisted of females, making the results more applicable to women, with unclear implications for older men. Additionally, the participants showed relatively good physical and cognitive abilities, as they completed questionnaires independently, which indicates good understanding and use of computers and the internet. The sample primarily consisted of individuals with better aging outcomes, and including those with more severe physical and cognitive limitations might have resulted in greater variability between successful and less successful aging, potentially revealing more prominent effects. The finding that only the compensation strategy moderated the relationship between chronic pain and depression may be related to the small sample size, as larger samples are recommended to detect minor effects (Aguinis et al., 2005). Regarding measurement instruments, while the Geriatric Depression Scale had adequate reliability, it lacked validity. Also, while the SOC questionnaire was reliable overall, due to the high correlations between the latent factors of the SOC scale, the overall construct validity of the scale appears to be limited. The Compensation scale was found to be lacking in both reliability and validity, thus raising concerns about its overall measurement quality. The sample size (N = 106) used for CFA was relatively small. Although recommendations for the CFA sample size vary, commonly cited guidelines suggest a minimum of 5 to 10 observations per estimated parameter or variable (Pakalniškienė, 2012; Hair et al., 2019). While our sample meets these criteria, it remains on the lower end of the recommended range.
Considering the study results and limitations, further research is needed to better understand the impact of successful aging on the relationship between chronic pain and depression. Future studies should use larger, more representative samples, as a bigger sample increases the likelihood of detecting moderating effects and is necessary for obtaining more reliable and stable CFA results. Meanwhile, inclusion of more individuals with lower successful aging outcomes could improve the accuracy of the findings. It is also essential to use more reliable and valid research instruments, though there is currently only one tool for measuring successful aging based on selection, optimization, and compensation strategies (Freund & Baltes, 2002). Expanding the research scope could involve exploring successful aging using alternative, as well as new(er) theories. Longitudinal studies are also necessary to identify causal relationships between chronic pain, depression, and successful aging.
Author contributions
Kamilė Naujalytė: conceptualization, formal analysis, investigation, methodology, validation, visualization, writing – original draft, writing – review and editing.
Rūta Sargautytė: conceptualization, methodology, supervision, validation, writing – review and editing.
References
Agüera-Ortiz, L., Failde, I., Cervilla, J. A., & Mico, J. A. (2013). Unexplained pain complaints and depression in older people in primary care. The Journal of Nutrition, Health & Aging, 17(6), 574–577. https://doi.org/10.1007/s12603-013-0012-0
Aguinis, H., Beaty, J. C., Boik, R. J., & Pierce, C. A. (2005). Effect size and power in assessing moderating effects of categorical variables using multiple regression: A 30–year review. The Journal of Applied Psychology, 90(1), 94–107. https://doi.org/10.1037/0021-9010.90.1.94
Alonso-Fernández, M., López–López, A., Losada, A., González, J. L., & Wetherell, J. L. (2016). Acceptance and commitment therapy and selective optimization with compensation for institutionalized older people with chronic pain. Pain Medicine (Malden, Mass.), 17(2), 264–277. https://doi.org/10.1111/pme.12885
Baltes, P. B., & Baltes, M. M. (1990). Psychological perspectives on successful aging: The model of selective optimization with compensation. In P. B. Baltes & M. M. Baltes (Eds.), Successful aging: Perspectives from the behavioral sciences (pp. 1–34). Cambridge University Press. https://doi.org/10.1017/CBO9780511665684.003
Baltes, P. B., Baltes, M. M., Freund, A. M., & Lang, F. R. (1999). The measurement of selection, optimization, and compensation (SOC) by self–report: Technical report. Max Planck Institute for Human Development, Berlin. https://doi.org/10.13140/RG.2.1.2213.4807
Baltes, M. M., & Carstensen, L. L. (1996). The process of successful ageing. Ageing and Society, 16(4), 397–422. https://doi.org/10.1017/S0144686X00003603
Bernfort, L., Gerdle, B., Rahmqvist, M., Husberg, M., & Levin, L. Å. (2015). Severity of chronic pain in an elderly population in Sweden – impact on costs and quality of life. Pain, 156(3), 521–527. https://doi.org/10.1097/01.j.pain.0000460336.31600.01
Chou, K. L., & Chi, I. (2001). Selection, Optimization, and Compensation Questionnaire: A validation study with Chinese older adults. Clinical Gerontologist: The Journal of Aging and Mental Health, 24(1–2), 141–152. https://doi.org/10.1300/J018v24n01_10
Deksnytė, A., Danilevičiūtė, V., Aranauskas, R., Gudynaitė, K., & Palinauskaitė, K. (2012). Somatinių pacientų depresiškumo nustatymas, naudojant Beko depresijos klausimyną ir geriatrinę depresijos skalę. Neurologijos seminarai, 16(52), 147–151. http://www.neuroseminarai.lt/wp-content/uploads/2017/02/Neuro_2012_Nr2_147-151.pdf
Domenichiello, A. F., & Ramsden, C. E. (2019). The silent epidemic of chronic pain in older adults. Progress in Neuro–Psychopharmacology & Biological Psychiatry, 93, 284–290. https://doi.org/10.1016/j.pnpbp.2019.04.006
Eurostat. (2024). Population structure and ageing. Eurostat. Retrieved December 17, 2024, from https://ec.europa.eu/eurostat/statistics-explained/SEPDF/cache/1271.pdf
Friedman, B., Heisel, M. J., & Delavan, R. L. (2005). Psychometric properties of the 15–item geriatric depression scale in functionally impaired, cognitively intact, community-dwelling elderly primary care patients. Journal of the American Geriatrics Society, 53(9), 1570–1576. https://doi.org/10.1111/j.1532-5415.2005.53461.x
Geldhof, G. J., Gestsdottir, S., Stefansson, K., Johnson, S. K., Bowers, E. P., & Lerner, R. M. (2015). Selection, optimization, and compensation: The structure, reliability, and validity of forced–choice versus Likert–type measures in a sample of late adolescents. International Journal of Behavioral Development, 39(2), 171–185. https://doi.org/10.1177/0165025414560447
Hair, J. F., Black, W. C., Babin, B. J., & Anderson, R. E. (2019). Multivariate Data Analysis (8th ed.). Cengage.
Janke, M., Son, J., & Payne, L. (2009). Self–regulation and adaptation of leisure activities among adults with arthritis. Activities, Adaptation & Aging, 33(2), 65–80. https://doi.org/10.1080/01924780902947058
Kairys, A., Zamalijeva, O., Bagdonas, A., Eimontas, J., Pakalniškienė, V., & Sadauskaitė, R. (2021). The well-being of older age Lithuanians: Policy implications. Psichologija, 65, 64–79. https://doi.org/10.15388/Psichol.2021.47
Kapos, F. P., Hancock, C., Guerrero Torres, V., Gonzalez Antonio, M. I., Do, A., & Jensen, M. P. (2023). Validation of the PEG scale in Spanish (PEG–S) among adults receiving care for pain in US primary care. The Journal of Pain, 24(11), 1897–1904. https://doi.org/10.1016/j.jpain.2023.06.005
Krebs, E. E., Lorenz, K. A., Bair, M. J., Damush, T. M., Wu, J., Sutherland, J. M., Asch, S. M., & Kroenke, K. (2009). Development and initial validation of the PEG, a three–item scale assessing pain intensity and interference. Journal of General Internal Medicine, 24(6), 733–738. https://doi.org/10.1007/s11606-009-0981-1
Liu, Z. H., Jin, Y., Rao, W. W., Zhang, Q., Zhang, J., Jackson, T., Su, Z., & Xiang, Y. T. (2021). The prevalence of painful physical symptoms in major depressive disorder: A systematic review and meta–analysis of observational studies. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 111, Article 110372. https://doi.org/10.1016/j.pnpbp.2021.110372
Meda, R. T., Nuguru, S. P., Rachakonda, S., Sripathi, S., Khan, M. I., & Patel, N. (2022). Chronic pain–induced depression: A review of prevalence and management. Cureus, 14(8), Article e28416. https://doi.org/10.7759/cureus.28416
Meng, A., Karlsen, I. L., Borg, V., & Clausen, T. (2022). Perceived collective use of selection, optimisation, and compensation: Associations with work ability. Nordic Journal of Working Life Studies, 13(1). https://doi.org/10.18291/njwls.132467
Moeller, M., & O’Brien, W. H. (2024). Integrating Acceptance and Commitment Therapy with Selective Optimization with Compensation to Predict Wellbeing. Clinical gerontologist, 1–13. https://doi.org/10.1080/07317115.2024.2432912
Nguyen, A. T., Nguyen, T. H. T., Nguyen, T. T. H., Nguyen, H. T. T., Nguyen, T. X., Nguyen, T. N., Nguyen, A. L., Vu, L. G., Do, H. T., Doan, L. P., Vu, G. T., Nguyen, H. T. T., Pham, T., & Vu, H. T. T. (2021). Chronic pain and associated factors related to depression among older patients in Hanoi, Vietnam. International Journal of Environmental Research and Public Health, 18(17), Article 9192. https://doi.org/10.3390/ijerph18179192
Nikitin, J., & Freund, A. M. (2019). The adaptation process of aging. In R. Fernandez–Ballesteros, J. M. Robine, & A. Benetos (Eds), The Cambridge Handbook of Successful Aging (pp. 281–298). Cambridge University Press.
Oficialiosios statistikos portalas. (2024). Lietuvos gyventojai. Gyventojų senėjimas. Retrieved December 17, 2024, from https://osp.stat.gov.lt/lietuvos-gyventojai-2023/salies-gyventojai/gyventoju-senejimas
Okabayashi, H. (2014). Development of a Japanese version of the selection, optimization, and compensation questionnaire. Journal of cross–cultural gerontology, 29(4), 447–465. https://doi.org/10.1007/s10823-014-9242-9
Pakalniškienė, V. (2012). Tyrimo ir įvertinimo priemonių patikimumo ir validumo nustatymas. Metodinė priemonė. Vilniaus universiteto leidykla.
Riedel, N., Müller, A., & Ebener, M. (2015). Applying strategies of selection, optimization, and compensation to maintain work ability – a psychosocial resource complementing the job demand-control model? Results from the representative lidA cohort study on work, age, and health in Germany. Journal of Occupational and Environmental Medicine, 57(5), 552–561. https://doi.org/10.1097/JOM.0000000000000402
Rikard, S. M., Strahan, A. E., Schmit, K. M., & Guy, G. P. Jr. (2023). Chronic pain among adults – United States, 2019–2021. MMWR. Morbidity and Mortality Weekly Report, 72(15), 379–385. https://doi.org/10.15585/mmwr.mm7215a1
Santos, J., Martins, S., Azevedo, L. F., & Fernandes, L. (2020). Pain as a risk factor for suicidal behavior in older adults: A systematic review. Archives of Gerontology and Geriatrics, 87, Article 104000. https://doi.org/10.1016/j.archger.2019.104000
Scur, M. D., Kampff, C. A., Antunes, D. C. R., Fey, S., Godoflite, M. C. S., Felitti, P. T. Q., & Alves dos Santos, G. (2021). Analysis of the relationship between depression and selection, optimization and compensation strategies in older people. International Journal of Development Research, 11(10), 50960–50962. https://doi.org/10.37118/ijdr.23185.10
Segura-Camacho, A., Rodríguez, F., Torre, L., & Topa, G. (2018). Successful aging at work: Psychometric properties of the Spanish version of Selection, Optimization and Compensation Questionnaire. Frontiers in Psychology, 9, 1–6. https://doi.org/10.3389/fpsyg.2018.00410
Sheikh, J. I., & Yesavage, J. A. (1986). Geriatric Depression Scale (GDS): Recent evidence and development of a shorter version. Clinical Gerontologist: The Journal of Aging and Mental Health, 5(1–2), 165–173. https://doi.org/10.1300/J018v05n01_09
Sheng, J., Liu, S., Wang, Y., Cui, R., & Zhang, X. (2017). The link between depression and chronic pain: Neural mechanisms in the brain. Neural Plasticity, 2017, Article 9724371. https://doi.org/10.1155/2017/9724371
Siren, A., & Hakamies–Blomqvist, L. (2009). Mobility and well–being in old age. Topics in Geriatric Rehabilitation, 25(1), 3–11. https://doi.org/10.1097/TGR.0b013e31819147bf
Viglund, K., Aléx, L., Jonsén, E., Lundman, B., Norberg, A., Fischer, R. S., Strandberg, G., & Nygren, B. (2013). Psychometric properties of the Swedish version of the Selection, Optimization, Compensation Questionnaire. Scandinavian Journal of Caring Sciences, 27(2), 460–467. https://doi.org/10.1111/j.1471-6712.2012.01027.x
Villar, F. (2012). Successful aging and development: The contribution of generativity in older age. Ageing & Society, 32(7), 1087–1105. https://doi.org/10.1017/S0144686X11000973
Warner, C. B., Roberts, A. R., Jeanblanc, A. B., & Adams, K. B. (2019). Coping resources, loneliness, and depressive symptoms of older women with chronic illness. Journal of Applied Gerontology, 38(3), 295–322. https://doi.org/10.1177/0733464816687218
Weber, J., Müller, A., Stiller, M., & Borchart, D. (2018). Prognostic effects of selection, optimization and compensation strategies on work ability: Results from the representative lidA cohort study on work, age, and health in Germany. International Archives of Occupational and Environmental Health, 91(8), 1061–1071. https://doi.org/10.1007/s00420-018-1348-x
World Health Organization. (2019). MG30 Chronic pain. In International statistical classification of diseases and related health problems (11th ed.). https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/1581976053
World Health Organization. (2024). Ageing and health. Retrieved December 17, 2024, from https://www.who.int/news-room/fact-sheets/detail/ageing-and-health
Zając-Lamparska, L. (2021). Selection, optimization and compensation strategies and their relationship with well–being and impulsivity in early, middle and late adulthood in a Polish sample. BMC Psychology, 9(1), Article 144. https://doi.org/10.1186/s40359-021-00650-2
Zhang, W., & Radhakrishnan, K. (2018). Evidence on selection, optimization, and compensation strategies to optimize aging with multiple chronic conditions: A literature review. Geriatric Nursing (New York, N.Y.), 39(5), 534–542. https://doi.org/10.1016/j.gerinurse
Zis, P., Daskalaki, A., Bountouni, I., Sykioti, P., Varrassi, G., & Paladini, A. (2017). Depression and chronic pain in the elderly: Links and management challenges. Clinical Interventions in Aging, 12, 709–720. https://doi.org/10.2147/CIA.S113576
Annex A
Figure A
Confirmatory factor analysis model of the chronic pain factors
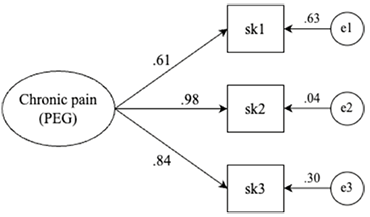
Note. All factor loadings are significant at p < 0.001.
Annex B
Figure B
Confirmatory factor analysis model of the depression factors
![[This figure is a structural equation model diagram representing a Confirmatory Factor Analysis (CFA) of depression, as measured by the Geriatric Depression Scale (GDS). At the top of the diagram is an oval labeled “Depression (GDS)”, representing a single latent factor. From this latent factor, 15 arrows point downward to 15 observed variables (rectangles labeled de1 to de15), indicating that all these variables load ontothe same latent construct. Each observed variable also has an associated measurement error shown as a small circle (labeled a1 to a15) with an arrow pointing to the corresponding observed variable. Standardized factor loadings (ranging approximately from 0.20 to 0.71) are displayed on the arrows connecting the latent variable to each observed indicator. Error variances are indicated between 0.50 and 0.96. Two covariances between error terms are shown at the bottom of the diagram: between a3 and a4, with a correlation of -0.40; and between a14 and a15, with a correlation of 0.37.
The note below says that all factor loadings are statistically significant at p < 0.05, except for item de10, which has a p-value of 0.055.]](https://www.zurnalai.vu.lt/psichologija/article/download/40090/version/36232/40522/124392/conf5.png)
Note. All factor loadings are significant at p < 0.05, except for item de10 (p = 0.055).
Annex C
Figure C
Confirmatory factor analysis model of the successful aging subscales
![[This figure presents a Confirmatory Factor Analysis (CFA) model of the successful aging subscales, as measured by The Selection, Optimization, and Compensation Questionnaire (SOC), which includes three latent constructs: Selection, Optimization, and Compensation. Each of these latent variables is depicted as an oval and is connected by straight arrows to their corresponding observed variables which are drawn as rectangles.
The latent variable Selection is associated with six observed variables: ss2, ss3, ss6, ss7, ss10, and ss11. These variables have standardized factor loadings of 0.66, 0.62, 0.61, 0.81, 0.55, and 0.65, respectively.
The latent factor Optimization is connected to three observed variables: ss1, ss5, and ss9, with standardized loadings of 0.64, 0.80, and 0.66, respectively.
The third latent variable, Compensation, is also associated with three observed variables: ss4, ss8, and ss12. These loadings are 0.63, 0.25, and 0.63, respectively.
Each observed variable is also linked to an error term, represented as a small circle and labeled x1 through x12.
Curved double-headed arrows represent correlations between the latent factors. The correlation between Selection and Optimization is 0.81, between Selection and Compensation is 1.05, and between Optimization and Compensation is 1.06. Additionally, there is a residual correlation of 0.28 between error terms x10 and x11.
The note below says that all factor loadings for the Selection and Optimization subscales are statistically significant at p < 0.001. Factor loadings for the Compensation subscale are statistically significant at p < 0.05.]](https://www.zurnalai.vu.lt/psichologija/article/download/40090/version/36232/40522/124388/fact6.png)
Note. All factor loadings for the Selection and Optimization subscales are significant at p < 0.001; factor loadings for the Compensation subscale are significant at p < 0.05.