Psichologija ISSN 1392-0359 eISSN 2345-0061
2026, vol. 74, pp. 8–23 DOI: https://doi.org/10.15388/Psichol.2026.74.1
Mapping the Interconnections Between Somatic Complaints, Mentalization and Stress Coping in Young Adulthood: A Network Analysis Approach
Aistė Treigytė
Vilnius University, Institute of Psychology
aiste.treigyte@fsf.stud.vu.lt
https://orcid.org/0009-0008-3771-8098
https://ror.org/03nadee84
Dovilė Mikučionytė
Vilnius University, Institute of Psychology
dovile.mikucionyte@fsf.stud.vu.lt
https://orcid.org/0009-0008-6990-9489
https://ror.org/03nadee84
Asta Adler
Vilnius University, Institute of Psychology
asta.zbarauskaite@fsf.vu.lt
https://orcid.org/0000-0003-1428-422X
https://ror.org/03nadee84
Abstract. Somatic complaints are highly prevalent among young adults and can significantly impair both psychological well-being and physical functioning. This study aimed to examine the associations between somatic complaints, mentalization, and stress coping strategies in young adults, a triad that remains underexplored in the current literature. A sample of 115 individuals (49 men, 66 women) aged 18–29 years completed an online survey assessing somatic complaints (Giessen Subjective Complaints List-24), mentalization (The Mentalization Scale, Dimitrijević et al., 2018), and stress coping strategies (Lithuanian Coping with Stress Questionnaire – Revised, Valickas et al., 2010). A network analysis approach was used to explore the complex interconnections among these constructs. Findings revealed that motivation to mentalize and self-oriented mentalization were the most central variables in the network, highlighting their importance in regulating stress and somatic symptoms. Notably, lower self-mentalization was strongly associated with greater somatic complaints and the use of maladaptive coping strategies. Somatic symptoms formed a densely connected subnetwork, with emotional venting emerging as the strongest directly linked maladaptive strategy. Conversely, adaptive coping strategies were positively associated with various dimensions of mentalization and appeared to buffer the impact of stress on somatic health. These results underscore the importance of self-reflective and motivational components of mentalization, as well as adaptive coping, in understanding and addressing somatic complaints. Enhancing these factors may offer promising therapeutic targets for interventions to reduce somatic symptom burden in young adults.
Keywords: somatic complaints, mentalization, stress coping, young adulthood.
Jaunų suaugusiųjų somatinių sunkumų, mentalizacijos ir streso įveikos strategijų sąsajos: tinklo analizė
Santrauka. Somatiniai sunkumai yra dažnas reiškinys jaunų suaugusiųjų gyvenime, kuris gali paveikti jų psichologinę gerovę bei fizinį funkcionavimą. Šiame tyrime buvo siekiama išnagrinėti somatinių sunkumų, mentalizacijos ir streso įveikos strategijų sąsajas jaunų suaugusiųjų imtyje – triadą, kuri menkai tyrinėta mokslinėje literatūroje. Tyrime dalyvavo 115 asmenų (49 vyrai ir 66 moterys), kurių amžius buvo nuo 18 iki 29 metų. Dalyviai pildė internetinę anketą, kurioje buvo vertinami somatiniai sunkumai (Giessen subjektyvių nusiskundimų sąrašas, Brähler et al., 2008), mentalizacijos gebėjimai (Mentalizacijos skalė, Dimitrijević et al., 2018) ir streso įveikos strategijos (Patobulintas keturių faktorių streso įveikos klausimynas, Valickas et al., 2010). Tyrime buvo taikytas tinklo analizės metodas, padedantis atskleisti šių konstrukcijų tarpusavio ryšius. Rezultatai parodė, kad motyvacija mentalizuoti ir į save nukreipta mentalizacija užėmė svarbiausias vietas tinkle, taip pabrėždamos jų reikšmę palaikant psichologinę ir fizinęsveikatą. Pastebėta, kad prastesni į save nukreiptos mentalizacijos gebėjimai buvo stipriai susiję su labiau išreikštais somatiniais sunkumais ir dažnesniu neadaptyvių įveikos strategijų taikymu. Somatiniai nusiskundimai sudarė glaudžiai susijusį potinklį, kuriame emocinė iškrova išryškėjo kaip stipriausiai su jais susijusi neadaptyvi įveikos strategija. Priešingai, adaptyvios įveikos strategijos buvo teigiamai susijusios su skirtingais mentalizacijos aspektais ir potencialiai silpnino streso poveikį fizinei sveikatai. Šie rezultatai pabrėžia į save nukreiptos mentalizacijos, motyvacijos mentalizuoti ir adaptyvių įveikų svarbą, siekiant geriau suprasti ir palengvinti somatinius sunkumus. Šių veiksnių stiprinimas gali veikti kaip perspektyvus terapinis tikslas jaunų suaugusiųjų somatinių sunkumų prevencijoje.
Pagrindiniai žodžiai: somatiniai sunkumai, mentalizacija, streso įveika, jauni suaugusieji.
Received: 2025-05-07. Accepted: 2025-06-27.
Copyright © 2025 Aistė Treigytė, Dovilė Mikučionytė, Asta Adler. Published by Vilnius University Press. This is an Open Access article distributed under the terms of the Creative Commons Attribution Licence (CC BY), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction
Somatic complaints are highly prevalent among young adults and can significantly impair both psychological well-being and physical functioning. These complaints are defined as subjectively experienced, unpleasant bodily sensations, such as headaches, back pain, and nausea, that lack a clear medical explanation (Brown, 2007). Previous studies across various countries have demonstrated the widespread nature of these symptoms in the young adult population. A study conducted in Lithuania by Kriaučionienė et al. (2013) found that only 36.5% of young men and 17.1% of young women reported no somatic difficulties in the preceding year. Similarly, Kerekes et al. (2021) reported that approximately 50% of Swedish young adults had experienced at least one somatic symptom in the past 14 days. Pronounced somatic difficulties during this developmental stage can lead to absenteeism from educational or occupational settings and reduce social engagement (Acevedo-Mesa et al., 2019). These complaints are also a frequent reason for outpatient medical consultations, often leading to frustration for patients and healthcare providers and increasing healthcare utilization and expenditures (Jadhakhan et al., 2022).
Notably, somatic complaints can range from normative to pathological manifestations. When somatic symptoms do not significantly interfere with daily functioning, they are considered a normative phenomenon of young adulthood (Feneberg et al., 2021). In contrast, more severe, persistent or disabling symptoms may indicate underlying conditions, such as somatoform disorders as classified in the ICD-10 (WHO, 2016) or somatic symptom disorders, as defined in DSM-5 (APA, 2013). Thus, somatic difficulties in young adults may represent both a natural developmental phenomenon and a potential component of pathology. The present study focuses on non-clinical expressions of somatic complaints in this population.
A growing body of literature links somatic complaints to elevated stress levels, which are especially salient during young adulthood - a life stage marked by developmental transitions, further identity formation, and increasing psychosocial demands (Cusack & Merchant, 2013). Across numerous studies (Lind et al., 2014; Reininger et al., 2023; Teixeira et al., 2022), stress has been consistently identified as a significant contributor to the development and persistence of somatic complaints. Chronic or unresolved stress has been shown to heighten bodily awareness and sensitivity to physical discomfort, thereby amplifying the perception and persistence of somatic symptoms (Lind et al., 2014; Reininger et al., 2023; Teixeira et al., 2022). Emerging evidence suggests that a range of psychological factors may contribute to how young adults manage developmental challenges and somatic complaints, with mentalization and stress coping strategies being among the potential contributors. However, the nature of these relationships remains complex and not yet fully understood (Spink et al., 2018), warranting further investigation.
Mentalization is a multifaceted psychological construct, defined as the capacity to understand, interpret, and explain both one’s own and others’ mental states, such as emotions, beliefs, desires, and intentions, by drawing on internal cues and externally observable behavior (Fonagy et al., 2004). This capacity encompasses two key dimensions: self-oriented mentalization, which involves reflecting on and regulating one‘s own inner experiences, and other-oriented mentalization, which relates to understanding the mental states of others (Fonagy et al., 2004). More recently, scholars have highlighted the motivational dimension of mentalization, referring to an individual‘s curiosity, willingness and effort to engage in mentalizing processes (Jańczak, 2021), particularly under conditions of emotional arousal or stress. Mentalization supports developing and maintaining interpersonal relationships and serves as a foundation for emotional self-regulation and behavioral control (Fonagy & Allison, 2012). Effective mentalizing is associated with greater psychological resilience and adaptive stress coping, which is particularly relevant given the developmental pressures of young adulthood (Ballespí et al., 2022; A. W. Bateman & Fonagy, 2013). Conversely, elevated stress levels have been shown to impair mentalization capacity, especially in situations requiring complex emotional processing or interpersonal sensitivity (Bateman & Fonagy, 2019). Therefore, the interplay between stress, mentalization, and coping strategies may critically influence both psychological outcomes and somatic symptomatology in young adults.
Stress coping strategies, defined as cognitive and behavioral efforts to resolve, tolerate, or mitigate the internal and external discomfort caused by stressful situations (Lazarus & Folkman, 1984), are also closely intertwined with mentalization. Valickas et al. (2010), drawing on the work of several authors (Amirkhan, 1994; Carver et al., 1989; Lazarus & Folkman, 1984; Parker & Endler, 1992), identified four primary coping strategies: problem-solving, seeking social support, emotional venting and avoidance. Problem-focused coping strategies are generally considered adaptive, as they aim to resolve the source of stress. In contrast, emotion-focused strategies, particularly involving avoidance or emotional venting, may be maladaptive in specific contexts, as it primarily modulates the emotional response, leaving the stressor underaddressed (Heckhausen et al., 2010). Research indicates that young adults with higher self-oriented mentalization are more likely to employ adaptive coping strategies in both acute and chronic stress situations (Luyten & Fonagy, 2014; Schwarzer et al., 2022) and less likely to rely on avoidance-oriented coping (McFarland & and Dixon, 2021). These associations may reflect the role of self-mentalization in supporting effective emotion regulation and the capacity to process distressing internal experiences, rather than disengage from them (Ballespí et al., 2019). In contrast, impairments in mentalization, particularly in the self-oriented dimension, are associated with heightened stress sensitivity and increased reliance on maladaptive coping strategies (Janik McErlean & Lim, 2020; Magai & Hunziker, 1993). Thus, well-developed mentalization may serve as a foundation for adaptive stress coping, whereas limited mentalizing capacity may contribute to less effective or maladaptive coping responses.
Empirical research also points to significant associations between somatic complaints and both mentalization and stress coping. Maladaptive coping strategies, particularly avoidance, have been consistently linked to an increased prevalence of somatic symptoms (Adriaenssens et al., 2012; Folkman et al., 1986; Hall et al., 2011; Lind et al., 2014). However, the directionality of these associations remains unclear. While some researchers argue that maladaptive coping may act as a risk factor for somatic complaints (Frølund Pedersen et al., 2016; Ogre et al., 2016), others contend that these coping strategies may develop in response to persistent somatic symptoms (Peterlin et al., 2011).
Moreover, difficulties in mentalization, particularly the self-oriented dimension, have been associated with increased somatic complaints (Luyten et al., 2012, 2013; Reininger et al., 2023). Individuals who struggle to identify or express negative emotional states tend to report more somatic symptoms (Ballespí et al., 2019, 2022; Petzke et al., 2024), and emotional suppression has been linked to increased physiological arousal, potentially reinforcing unpleasant somatic sensations (Gupta & Pérez-Edgar, 2012; Raffagnato et al., 2020). While these findings indicate important relationships between somatic complaints, mentalization, and coping strategies, the nature of the interactions among all three constructs remains complex and insufficiently understood.
Although existing research highlights relevant associations among these constructs, studies examining the interrelations among mentalization, stress coping strategies, and somatic complaints, specifically in young adults, remain scarce, revealing a notable gap in the literature. Most studies focus on general mentalizing capacity (Castellini et al., 2024; Jansen et al., 2023; Schwarzer et al., 2022) or self-oriented mentalization (Schwarzer et al., 2021; Sonnby-Borgström, 2009), with limited attention to other-oriented mentalization or the motivation to mentalize dimension with stress coping or somatic symptoms. Furthermore, the majority of previous research has investigated only two of the three constructs examined in this study, and often using samples drawn from children, adolescents (Bizzi et al., 2022; Mazzone & Camodeca, 2018) or broader adult populations (Frølund Pedersen et al., 2016; Luyten & Fonagy, 2020). To date, no studies have comprehensively examined the interrelations among mentalization, stress coping strategies, and somatic difficulties specifically in young adulthood. Addressing this gap, the present study aims to investigate the relationship among these three constructs within a sample of young adults.
Current study
To address the gap in the literature, network analysis was selected as the methodological approach. Given that the interrelations among somatic complaints, mentalization, and stress coping strategies remain largely unexplored, network analysis provides a valuable framework for examining the complex, multidimensional associations among these constructs. By mapping these interconnections, the study aims to generate a more comprehensive understanding of the mechanisms underlying somatic complaints. In addition to exploring the overall structure of the network, this study specifically investigates the role of mentalization dimensions and coping strategies. It is hypothesized that better self-oriented mentalization and the use of problem-solving coping strategies will emerge as central, potentially protective factors in the network, associated with fewer somatic complaints. In contrast, avoidance coping is expected to function as a contributing factor to increased somatic symptoms.
Methods
Participants and Procedure
A total of 115 young adults residing in Lithuania participated in this study, including 49 males (42.6%) and 66 females (57.4%). Participants ranged in age from 18 to 29 years (M = 24.43; SD = 3.35). Recruitment was conducted via the social media platform Facebook, where individuals within a specified age range were invited to complete an anonymous online survey. Participation was voluntary, and no remuneration was provided. Before the survey, all participants provided informed consent, encompassing the information about the purpose of the study, the guarantees of anonymity and confidentiality, and their right to withdraw at any time. Participants were also provided with the researchers‘ contact details for any questions. Subsequently, they completed the online survey using Microsoft Forms.
Measures
Somatic Complaints: The Lithuanian version of the Giessen Subjective Complaints List-24 (GBB-24; Brähler et al., 2008) was used to assess somatic complaints. This self-report measure consists of 24 items covering various somatic complaints (e.g. nausea, head pressure, weariness, pains in neck or shoulders) experienced by the respondent during the last 7 days. Each item is rated on a four-point Likert scale ranging from 0 („not at all“) to 4 („very much“). The total score was calculated by summing the responses, with higher scores indicating greater somatic symptom severity.
The authors of the present study translated the GBB-24 into Lithuanian following a double translation and back-translation procedure with permission granted by Prof. Dr. A. Hinz. The original version of this scale has demonstrated good validity and reliability (Cronbach’s α = 0.94) (Brähler et al., 2008). In the present study, the Lithuanian version showed similarly strong internal reliability, with Cronbach’s alpha of 0.93.
Mentalization: Mentalizing capacity was measured using the Lithuanian version of The Mentalization Scale (MentS; Dimitrijević et al., 2018). The Centre for Research in Developmental Psychopathology at Vilnius University provided translation with permission for research use. The MentS consists of 28 self-report items, divided into three subscales: other-oriented mentalization (MentS-O), self-oriented mentalization (MentS-S), and motivation to mentalize (MentS-M). The scale utilizes a five-point Likert scale ranging from 1 („completely incorrect“) to 5 („completely correct“). The total and subscale scores were derived by summing the responses, with higher scores indicating a more developed mentalizing capacity.
The original scale has demonstrated strong construct and criterion validity and reliability, along with satisfactory internal consistency in both clinical and non-clinical samples (Cronbach’s α = 0.75 and 0.84, respectively) (Dimitrijević et al., 2018). For the subscales, Cronbach’s alphas in the non-clinical sample were 0.74 (MentS-O), 0.77 (MentS-S), and 0.74 (MentS-M) (Dimitrijević et al., 2018). In the current study, internal consistency for the Lithuanian version was similarly high: α = 0.85 for the total scale, with subscale values of α = 0.76 for MentS-O, α = 0.80 for MentS-S, and α = 0.77 for MentS-M, supporting its reliability in this population.
Stress Coping Strategies: Stress coping strategies were assessed using the Lithuanian Coping with Stress Questionnaire – Revised (LCSQ–R; Valickas et al., 2010). This 24-item self-report questionnaire consists of four subscales: problem-solving (analyzing the issue, seeking and planning its solution, acquiring necessary knowledge), social support (seeking emotional and instrumental help from others), avoidance (aims to divert attention from the stressor or reinterpret it positively), and emotional venting (focuses on attributing blame and releasing negative emotions). Each subscale comprises six items rated on a five-point Likert scale, ranging from 1 (“never”) to 5 (“always”). The subscale scores were calculated by summing the responses, with higher scores reflecting the greater use of the specific coping strategy.
This instrument has demonstrated satisfactory psychometric properties. Valickas et al. (2010) showed that in the original validation study, Cronbach’s alpha values were 0.76 for the problem-solving, 0.86 for the social support, 0.66 for the avoidance, and 0.69 for the emotional venting. In the current study, Cronbach’s alphas were as follows: 0.73 for problem-solving, 0.87 for social support, 0.72 for emotional venting, and 0.61 for avoidance, indicating acceptable internal consistency in this sample.
Data Analysis
Descriptive statistics and correlation analyses were conducted using IBM SPSS v.26.0 software. The normality of data distribution was assessed for all study variables. The scores of the MentS, the GBB-24 and two subscales (Avoidance and Social support) of the LCSQ–R followed a normal distribution (Shapiro-Wilk and Kolmogorov–Smirnov tests were insignificant with p < 0.05). For the remaining two subscales (Problem-solving and Emotional venting) of the Improved Four-Factor Coping with Stress Questionnaire, normality was supported by skewness and kurtosis values within the acceptable range (±1; George & Mallery, 2016), as well as visual inspections of histograms and Q-Q plots, which indicated approximately Gaussian distribution. Based on these findings, parametric statistical criteria were used. The Pearson correlation coefficient was used to evaluate the relationships between the two variables.
Network analysis was conducted using JASP v.0.19.3 software. A Gaussian Graphical Model (GGM) was estimated using the Extended Bayesian Information Criterion graphical LASSO (EBICglasso) algorithm, with the tuning parameter (γ) set to 0.5, balancing model parsimony and sensitivity. The network included eight nodes, representing the three MentS subscales, four stress coping strategy subscales, and the total somatic complaints score. Edges reflect regularized partial correlations between nodes: blue edges indicate positive relationships, and red edges represent negative ones. The thickness of each edge corresponds to the strength of the partial correlation.
Node centrality was assessed using strength, closeness, and betweenness metrics. Expected influence was also calculated to capture the overall effect of each node. Clustering coefficients (Barrat, Onnela, WS, and Zhang) were used to evaluate local connectivity within the network.
Results
Descriptive statistics
Table 1 presents the descriptive statistics for all study variables. Participants reported relatively high levels of other-oriented mentalization (M = 39.23, SD = 4.58) and motivation to mentalize (M = 39.84, SD = 4.46), with scores nearing the upper end of the respective scales. Self-oriented mentalization yielded a lower mean score (M = 25.92, SD = 6.20; scale range 8–40), suggesting greater variability and potentially less developed self-mentalizing in the sample. Among coping strategies, problem solving was the most frequently used strategy (M = 21.86, SD = 3.69), followed by social support (M = 20.63, SD = 4.82), avoidance (M = 18.85, SD = 3.45), and emotional venting (M = 14.23, SD = 4.03). These findings indicate a general preference for more adaptive coping strategies. Expression of somatic complaints ranged from 5 to 72 on a 0–96 scale. The mean score of 28.62 for somatic complaints is closer to the lower end of the scale.
Table 1
Descriptive statistics
|
Variable |
Scale |
Scale |
Min. |
Max. |
M |
SD |
|---|---|---|---|---|---|---|
|
Other-oriented mentalization |
10 |
50 |
26 |
50 |
39.23 |
4.58 |
|
Self-oriented mentalization |
8 |
40 |
10 |
39 |
25.92 |
6.20 |
|
Motivation to mentalize |
10 |
50 |
28 |
49 |
39.84 |
4.46 |
|
Social Support |
6 |
30 |
6 |
30 |
20.63 |
4.82 |
|
Problem Solving |
6 |
30 |
12 |
30 |
21.86 |
3.69 |
|
Emotional Venting |
6 |
30 |
6 |
24 |
14.23 |
4.03 |
|
Avoidance |
6 |
30 |
10 |
28 |
18.85 |
3.45 |
|
Somatic Complaints |
0 |
96 |
5 |
72 |
28.62 |
15.20 |
M – arithmetic mean, SD – standard deviation, Min. – minimum, Max. – maximum
Pearson’s correlation coefficients were calculated to examine the associations among study variables (Table 2). Somatic complaints demonstrated significant associations with two of the four stress coping strategies. Specifically, somatic complaints were positively correlated with emotional venting (r = 0.347, p < 0.01) and negatively correlated with problem solving (r = -0.206, p < 0.05). Regarding mentalization, somatic complaints showed significant associations only with the self-oriented dimension (r = -0.494, p < 0.01).
Adaptive coping strategies showed consistent positive associations with various dimensions of mentalization. Problem-solving was significantly positively correlated with all three dimensions: other-oriented mentalization (r = 0.491, p < 0.01), motivation to mentalize (r = 0.568, p < 0.01), and self-oriented mentalization (r = 0.324, p < 0.01). Similarly, social support was positively associated with other-oriented mentalization (r = 0.396, p < 0.01) and motivation to mentalize (r = 0.436, p < 0.01).
In contrast, self-oriented mentalization was negatively associated with both maladaptive stress coping strategies: emotional venting (r = -0.497, p < 0.01) and avoidance (r = -0.188, p < 0.05), suggesting that individuals with lower self-oriented mentalizing abilities are more likely to engage in maladaptive coping strategies.
Table 2
Correlation matrix of study variables
|
Variable |
1. |
2. |
3. |
4. |
5. |
6. |
7. |
8. |
|---|---|---|---|---|---|---|---|---|
|
1. Somatic Complaints |
1 |
|
|
|
|
|
|
|
|
2. Social Support |
-.153 |
1 |
|
|
|
|
|
|
|
3. Problem Solving |
-.206* |
.372** |
1 |
|
|
|
|
|
|
4. Emotional Venting |
.347** |
.099 |
-.167 |
1 |
|
|
|
|
|
5. Avoidance |
-.001 |
.313** |
.225* |
.212* |
1 |
|
|
|
|
6. Other-oriented mentalization |
-.052 |
.396** |
.491** |
-.103 |
.137 |
1 |
|
|
|
7. Motivation to mentalize |
-.060 |
.436** |
.568** |
-.150 |
-.007 |
.570** |
1 |
|
|
8. Self-oriented mentalization |
-.494** |
.156 |
.324** |
-.497** |
-.188* |
.198* |
.324** |
1 |
* Correlation is significant at the 0.05 level; ** Correlation is significant at the 0.01 level
Network estimation
A partial correlation network analysis was conducted to explore the associations among somatic complaints, dimensions of mentalization, and coping strategies in a sample of young adults. The network included eight nodes and revealed 15 non-zero edges out of a possible 28, resulting in a sparsity of 0.464. This indicates a moderately connected network, allowing for the identification of distinct clusters and central processes. The graphical representation of the network is illustrated in Figure 1.
Figure 1
Network of somatic complaints, mentalization and coping strategies
![A circular network graph visualizing the partial correlations between eight study variables. Each variable is represented as a numbered node: 1) Coping: Avoidance, 2) Coping: Emotional Venting, 3) Coping: Problem Solving, 4) Coping: Social Support, 5) Motivation to Mentalize, 6) Other-oriented Mentalization, 7) Self-oriented Mentalization and 8) Somatic Complaints. Edges (lines between nodes) represent partial correlations between study variables. Blue lines indicate positive, and red lines indicate negative partial correlations. Thicker and darker lines indicate stronger partial correlations. Thinner or lighter-colored lines indicate weak associations.]](https://www.zurnalai.vu.lt/psichologija/article/download/41859/version/38001/40518/124375/netwis1.png)
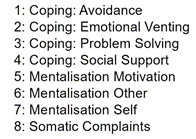
The analysis of the partial correlation coefficients and the visual inspection of the network model indicated that somatic complaints were most strongly negatively connected to self-oriented mentalization (r=-0.3) and weakly positively connected to emotional venting coping strategy (r=0.09). Self-oriented mentalization, in turn, had a weak positive relation with motivation to mentalize (r=0.1), and problem-solving (r=0.1) and weak negative associations with avoidant (r=-0.03) coping strategy.
Among mentalization dimensions, motiva tion to mentalize was weakly positively related to both self-oriented and other-oriented mentalization; however, the latter two were not directly connected, indicating distinct and separate roles within the network.
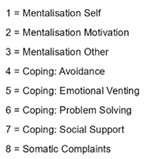
Figure 2 depicts centrality indices in terms of betweenness, closeness, strength and expected influence. Among all nodes, motivation to mentalize and self-oriented mentalization demonstrated the highest centrality indices. Motivation to mentalize showed high betweenness (1.288), closeness (1.634), strength (1.305), and expected influence (1.222). Self-oriented mentalization also exhibited a high betweenness (1.790) and strength (1.217), though its expected influence was negative (–1.445). Conversely, somatic complaints, avoidance, and emotional venting coping strategies showed consistently low centrality across all indices, indicating weak connectivity to the network. Other variables, including problem-solving, other-oriented mentalization, and social support, showed moderate centrality.
Figure 2
Centrality measures of somatic complaints, mentalization and coping strategies
![A figure consists of four side-by-side line plots, each displaying one centrality metric: betweenness, closeness, strength, and expected influence. All plots share the same vertical axis, listing eight study variables: from top to bottom: Self-oriented Mentalization, Motivation to Mentalize, Other-oriented Mentalization, Coping: Avoidance, Coping: Emotional Venting, Coping: Problem Solving, Coping: Social Support and Somatic Complaints.]](https://www.zurnalai.vu.lt/psichologija/article/download/41859/version/38001/40518/124377/centrlis2.png)
Clustering metrics are presented in Table 3. Somatic complaints and other-oriented mentalization showed the highest clustering across all four methods, suggesting that variables connected to somatic complaints or other-oriented mentalization also tend to be connected to each other. The weakest clustered variables were self-oriented mentalization and avoidance coping strategy. Negative clustering values across metrics indicate dispersion and limited integration into cohesive subgroups.
Table 3
Clustering coefficients
|
Variable |
Barrat |
Onnela |
WS |
Zhang |
|---|---|---|---|---|
|
Somatic Complaints |
1.25 |
1.54 |
1.46 |
1.84 |
|
Social Support |
-0.34 |
-0.26 |
-0.10 |
-0.23 |
|
Problem Solving |
-0.32 |
-0.44 |
-0.41 |
-0.06 |
|
Emotional Venting |
0.57 |
-0.24 |
-0.10 |
0.41 |
|
Avoidance |
-1.18 |
-1.20 |
-0.87 |
-1.14 |
|
Mentalization Other |
1.25 |
1.34 |
1.46 |
0.75 |
|
Mentalization Motivation |
0.15 |
0.26 |
-0.10 |
-0.39 |
|
Mentalization Self |
-1.38 |
-1.01 |
-1.34 |
-1.18 |
In summary, the network analysis identified self-oriented mentalization and motivation to mentalize as the most central variables, based on multiple centrality indices. Somatic complaints, along with avoidance and emotional venting coping strategies, showed low centrality, suggesting limited connectivity within the network. Clustering analysis indicated that somatic complaints and other-oriented mentalization were part of more interconnected clusters, while self-oriented mentalization and avoidance showed lower clustering coefficients.
Discussion
This study applied network analysis to investigate the interrelations between somatic complaints, mentalization dimensions, and stress coping strategies in young adults. The findings provide insight into psychological constructs most central to the network and their potential influence on somatic symptoms.
Two mentalization dimensions: motivation to mentalize and self-oriented mentalization, emerged as central nodes in the network. These findings suggest that young adults’ motivation to engage in understanding mental states, along with their capacity to reflect on their own internal experiences, play a pivotal role in the broader network of stress coping and somatic symptom experience. Notably, self-oriented mentalization demonstrated a strong negative expected influence, indicating that lower self-reflective capacities may be directly associated with heightened somatic complaints and the greater use of maladaptive coping strategies. The data suggest that self-oriented mentalizing ability is associated with emotion regulation, potentially allowing individuals to process stress more adaptively and avoid somatization. This finding aligns with prior research highlighting the role of impaired self-oriented mentalization in coping with stress (Ballespí et al., 2019; Janik McErlean & Lim, 2020; Luyten et al., 2012).
Interestingly, self-oriented and other-oriented mentalization appeared to function through distinct pathways, reinforcing the conceptualization of these components as partially independent processes (Fonagy et al., 2004; Luyten et al., 2013). While other-oriented mentalization was positively associated with adaptive coping strategies, particularly problem-solving, it did not demonstrate a direct relationship with somatic symptoms. This pattern is consistent with previous findings suggesting that other-mentalization is more strongly tied to interpersonal functioning and social regulation (Bateman & Fonagy, 2013), rather than directly influencing somatic symptom expression (Ballespí et al., 2022).
These results are also in line with earlier work by Schwarzer et al. (2021, 2022), which emphasized the protective role of self-oriented mentalization in stress management, as well as studies linking problem-solving strategies to more favorable psychological outcomes and avoidance to increased somatic complaints (Adriaenssens et al., 2012; Lind et al., 2014). Importantly, our findings extend this body of research by integrating all three constructs—mentalization, stress coping, and somatic symptoms—within a single model, and identifying motivation to mentalize as a central component in these associations, potentially buffering against maladaptive outcomes.
Somatic complaints were found to cluster tightly, suggesting that they form a distinct and highly interconnected subnetwork within the broader psychological profile of young adults. The strongest direct associations were observed between somatic complaints and emotional venting - a maladaptive, emotion-focused coping strategy. This finding supports earlier research indicating that coping strategies involving emotional discharge, without active problem resolution, may contribute to the intensification and persistence of somatic symptoms (Adriaenssens et al., 2012; Hall et al., 2011). The negative association between somatic complaints and self-oriented mentalization align with previous research suggesting that deficits in self-awareness and emotional insight may underlie increased somatic symptom reporting (Ballespí et al., 2019; Petzke et al., 2024).
Among coping strategies, both problem-solving and seeking social support demonstrated positive associations with mentalization dimensions. These results suggest that the ability to mentalize about one’s own and others’ internal states may facilitate more adaptive stress regulation strategies. These findings are consistent with prior studies indicating that individuals with stronger mentalizing capacities are more likely to engage in constructive coping mechanisms (McFarland & and Dixon, 2021; Schwarzer et al., 2022). In contrast, emotional venting was negatively related to self-oriented mentalization and positively linked to somatic complaints, underscoring its maladaptive role in this context. This supports the notion that ineffective stress coping, together with poor self-mentalization, can exacerbate physical symptomatology.
Moreover, network clustering coefficients revealed that adaptive coping strategies, particularly problem-solving and social support, were more deeply embedded in the overall network structure. This suggests that they may serve as protective nodes, potentially buffering the impact of stress on somatic health. In contrast, avoidance coping showed minimal connectivity and low centrality, indicating a more peripheral and possibly passive role in the coping process for this population. While previous literature identifies avoidance as a risk factor for somatic complaints (Lind et al., 2014), its weak integration within the current network may reflect contextual differences or individual variability in how avoidance is expressed among young adults.
Taken together, these findings contribute to a nuanced understanding of how mentalization capacities and specific coping strategies interact with somatic complaints, emphasizing the importance of self-reflection and motivational engagement. They also highlight the utility of network analysis in capturing these complex dynamics in a multidimensional framework.
In conclusion, the results highlight mentalization, especially motivational and self-oriented dimensions, as potential targets for intervention in efforts to reduce stress-related somatic complaints in young adults. Interventions that enhance the motivation to understand mental states in self and others, as well as the capacity to mentalize about one‘s mental states, could foster more effective stress coping and reduce somatic symptom expression. Strengthening adaptive coping strategies such as problem-solving and social support, while discouraging reliance on emotional venting, may offer additional benefits in managing stress and its physical manifestations.
Limitations and Future Directions
Despite the valuable insights provided by this study, several limitations should be acknowledged. First, the cross-sectional design precludes any conclusions about the directionality or causality of the observed relationships. Longitudinal designs are warranted to examine how somatic complaints, mentalization, and coping strategies interact. Second, the findings are based on a non-clinical sample of young adults, which may limit their generalizability to clinical populations; replication in samples with diagnosed somatic symptom disorders is needed to assess the robustness of the network structure. Additionally, the use of an online questionnaire may have introduced sampling bias and limited control over response conditions, potentially affecting data quality due to misunderstandings or lack of clarification. Third, while the network analysis captures complex multivariate associations, it is sensitive to sample size. Future research should aim to replicate these findings with larger samples. Finally, future intervention studies should explore whether enhancing mentalization abilities, particularly self-oriented and motivational components, improves stress coping and reduces somatic complaints in young adults.
Author contributions
Aistė Treigytė: conceptualization, data curation, formal analysis, investigation, methodology, writing – original draft, writing – review & editing.
Dovilė Mikučionytė: conceptualization, formal analysis, methodology, project administration, writing – original draft, writing – review & editing.
Asta Adler: conceptualization, formal analysis, methodology, project administration, supervision, writing – review & editing.
References
Acevedo-Mesa, A., Rosmalen, J. G. M., Ranchor, A. V., & Roest, A. M. (2019). Positive affect and functional somatic symptoms in young adults. Journal of Psychosomatic Research, 127, Article 109847. https://doi.org/10.1016/j.jpsychores.2019.109847
Adriaenssens, J., de Gucht, V., & Maes, S. (2012). The impact of traumatic events on emergency room nurses: Findings from a questionnaire survey. International Journal of Nursing Studies, 49(11), 1411–1422. https://doi.org/10.1016/j.ijnurstu.2012.07.003
American Psychiatric Association, DSM-5 Task Force. (2013). Diagnostic and statistical manual of mental disorders: DSM-5™ (5th ed.). American Psychiatric Publishing. https://doi.org/10.1176/appi.books.9780890425596
Ballespí, S., Nonweiler, J., Sharp, C., Vives, J., & Barrantes-Vidal, N. (2022). Self- but not other-mentalizing moderates the association between BPD symptoms and somatic complaints in community-dwelling adolescents. Psychology and Psychotherapy: Theory, Research and Practice, 00(n/a), 1–16. https://doi.org/10.1111/papt.12409
Ballespí, S., Vives, J., Alonso, N., Sharp, C., Ramírez, M. S., Fonagy, P., & Barrantes-Vidal, N. (2019). To know or not to know? Mentalization as protection from somatic complaints. PLoS ONE, 14(5), Article e0215308. https://doi.org/10.1371/journal.pone.0215308
Bateman, A. W., & Fonagy, P. (2013). Mentalization-Based Treatment. Psychoanalytic Inquiry, 33(6), 595–613. https://doi.org/10.1080/07351690.2013.835170
Bateman, A. W., & Fonagy, P. (2019). Handbook of Mentalizing in Mental Health Practice. American Psychiatric Pub.
Bizzi, F., Mora, S. C., Tironi, M., Riva, A., & Nacinovich, R. (2022). Multimethod Assessment of Mentalizing and its relations with Somatic Symptoms in Adolescents with Primary Headache. European Psychiatry, 65(S1), S442–S442. https://doi.org/10.1192/j.eurpsy.2022.1122
Brown, R. J. (2007). Introduction to the special issue on medically unexplained symptoms: Background and future directions. Clinical Psychology Review, 27(7), 769–780. https://doi.org/10.1016/j.cpr.2007.07.003
Brähler, E., Hinz, A., & Scheer, J. W. (2008). GBB-24. Der Gießener Beschwerdebogen. Manual, 3.
Castellini, G., Tarchi, L., Cassioli, E., Ricca, V., Abbate Daga, G., Aguglia, A., Albert, U., Atti, A., Barlati, S., Blasi, G., Carmassi, C., Carrà, G., De Fazio, P., De Panfilis, C., Di Lorenzo, G., Ferrari, S., Goracci, A., Gramaglia, C., Luciano, M., … Fiorillo, A. (2024). The interplay between mentalization, personality traits and burnout in psychiatry training: Results from a large multicenter controlled study. Acta Psychiatrica Scandinavica, 149(3), 177–194. https://doi.org/10.1111/acps.13649
Cusack, C., & Merchant, C. (2013). The effects of emerging adulthood on stress and depression. Modern Psychological Studies, 18(2), 47–64. https://scholar.utc.edu/mps/vol18/iss2/6
Dimitrijević, A., Hanak, N., Altaras Dimitrijević, A., & Jolić Marjanović, Z. (2018). The Mentalization Scale (MentS): A Self-Report Measure for the Assessment of Mentalizing Capacity. Journal of Personality Assessment, 100(3), 268–280. https://doi.org/10.1080/00223891.2017.1310730
Feneberg, A. C., Mewes, R., Doerr, J. M., & Nater, U. M. (2021). The effects of music listening on somatic symptoms and stress markers in the everyday life of women with somatic complaints and depression. Scientific Reports, 11(1), Article 24062. https://doi.org/10.1038/s41598-021-03374-w
Folkman, S., Lazarus, R. S., Gruen, R. J., & DeLongis, A. (1986). Appraisal, coping, health status, and psychological symptoms. Journal of Personality and Social Psychology, 50(3), 571–579. https://doi.org/10.1037/0022-3514.50.3.571
Fonagy, P., & Allison, E. (2012). What is mentalization? The concept and its foundations in developmental research. In N. Midgley & I. Vrouva (Eds.), Minding the child: Mentalization-based interventions with children, young people and their families (pp. 11–34). Routledge/Taylor & Francis Group.
Fonagy, P., Gergely, G., Jurist, E. L., & Target, M. (2004). Affect Regulation, Mentalization, and the Development of Self. Other Press. https://www.amazon.com/Affect-Regulation-Mentalization-Development-Self/dp/1590511611
Frølund Pedersen, H., Frostholm, L., Søndergaard Jensen, J., Ørnbøl, E., & Schröder, A. (2016). Neuroticism and maladaptive coping in patients with functional somatic syndromes. British Journal of Health Psychology, 21(4), 917–936. https://doi.org/10.1111/bjhp.12206
George, D., & Mallery, P. (2016). IBM SPSS Statistics 23 Step by Step: A Simple Guide and Reference (14th ed.). Routledge. https://doi.org/10.4324/9781315545899
Gupta, D., & Pérez-Edgar, K. (2012). The role of temperament in somatic complaints among young female adults. Journal of Health Psychology, 17(1), 26–35. https://doi.org/10.1177/1359105311405351
Hall, N. M., Kuzminskyte, R., Pedersen, A. D., Ørnbøl, E., & Fink, P. (2011). The relationship between cognitive functions, somatization and behavioural coping in patients with multiple functional somatic symptoms. Nordic Journal of Psychiatry, 65(3), 216–224. https://doi.org/10.3109/08039488.2010.528024
Heckhausen, J., Wrosch, C., & Schulz, R. (2010). A motivational theory of life-span development. Psychological Review, 117(1), 32–60. https://doi.org/10.1037/a0017668
Jadhakhan, F., Romeu, D., Lindner, O., Blakemore, A., & Guthrie, E. (2022). Prevalence of medically unexplained symptoms in adults who are high users of healthcare services and magnitude of associated costs: A systematic review. BMJ Open, 12(10), Article e059971. https://doi.org/10.1136/bmjopen-2021-059971
Jańczak, M. O. (2021). Polish adaptation and validation of the Mentalization Scale (MentS)—A self-report measure of mentalizing. Psychiatria Polska, 55(6), 1257–1274. https://doi.org/10.12740/PP/125383
Janik McErlean, A. B., & Lim, L. X. C. (2020). Relationship between Parenting Style, Alexithymia and Aggression in Emerging Adults. Journal of Family Issues, 41(6), 853–874. https://doi.org/10.1177/0192513X19886647
Jansen, N., Kühl, J., Eller, N., Kingdon, P., & Firk, C. (2023). Mentalizing Capacity Partially Mediates the Relationship Between Attachment and Stress, Depression, and Anxiety in Social Work Students. Clinical Social Work Journal, 51(4), 339–353. https://doi.org/10.1007/s10615-023-00882-2
Kerekes, N., Zouini, B., Tingberg, S., & Erlandsson, S. (2021). Psychological Distress, Somatic Complaints, and Their Relation to Negative Psychosocial Factors in a Sample of Swedish High School Students. Frontiers in Public Health, 9, Article 669958. https://doi.org/10.3389/fpubh.2021.669958
Kriaučionienė, V., Barkauskienė, A., & Petkevičienė, J. (2013). Kauno universitetų studentų subjektyvi sveikata ir jos pokyčiai 2000–2010 m. Visuomenės sveikata, 2(61), 82–88.
Lazarus, R. S., & Folkman, S. (1984). Stress, Appraisal, and Coping (1st ed.). Springer Publishing Company.
Lind, A. B., Delmar, C., & Nielsen, K. (2014). Struggling in an emotional avoidance culture: A qualitative study of stress as a predisposing factor for somatoform disorders. Journal of Psychosomatic Research, 76(2), 94–98. https://doi.org/10.1016/j.jpsychores.2013.11.019
Luyten, P., & Fonagy, P. (2014). Mentalising in attachment contexts. In P. Holmes & S. Farnfield (Eds.), The Routledge handbook of attachment: Theory (pp. 109–126). Routledge/Taylor & Francis Group. https://doi.org/10.4324/9781315762098
Luyten, P., & Fonagy, P. (2020). Psychodynamic Psychotherapy for Patients with Functional Somatic Disorders and the Road to Recovery. American Journal of Psychotherapy, 73(4), 125–130. https://doi.org/10.1176/appi.psychotherapy.20200010
Luyten, P., van Houdenhove, B., Lemma, A., Target, M., & Fonagy, P. (2012). A mentalization-based approach to the understanding and treatment of functional somatic disorders. Psychoanalytic Psychotherapy, 26(2), 121–140. https://doi.org/10.1080/02668734.2012.678061
Luyten, P., Van Houdenhove, B., Lemma, A., Target, M., & Fonagy, P. (2013). Vulnerability for functional somatic disorders: A contemporary psychodynamic approach. Journal of Psychotherapy Integration, 23(3), 250–262. https://doi.org/10.1037/a0032360
Magai, C., & Hunziker, J. (1993). Tolstoy and the riddle of developmental transformation: A lifespan analysis of the role of emotions in personality development. In M. Lewis & J. M. Haviland (Eds.), Handbook of emotions (pp. 247–259). The Guilford Press.
Mazzone, A., & Camodeca, M. (2018). Emotion awareness and somatic complaints in preadolescence: The mediating role of coping strategies. Infant and Child Development, 27(3), Article e2075. https://doi.org/10.1002/icd.2075
McFarland, R. G., & Dixon, A. L. (2021). The impact of salesperson interpersonal mentalizing skills on coping and burnout: The critical role of coping oscillation. Journal of Personal Selling & Sales Management, 41(4), 285–300. https://doi.org/10.1080/08853134.2021.1898412
Ogre, S. C., Chakravarty, M., Shrivastava, P., & Janghel, G. (2016). Relationship between somatic problems and their coping strategies among sickle cell anaemic adolescents. Indian Journal of Health and Wellbeing, 7(5), 510–513.
Peterlin, B. L., Rosso, A. L., Sheftell, F. D., Libon, D. J., Mossey, J. M., & Merikangas, K. R. (2011). Post-traumatic stress disorder, drug abuse and migraine: New findings from the National Comorbidity Survey Replication (NCS-R). Cephalalgia : An International Journal of Headache, 31(2), 235–244. https://doi.org/10.1177/0333102410378051
Petzke, T. M., Weber, K., Van den Bergh, O., & Witthöft, M. (2024). Illustrating the pathway from affect to somatic symptom: The Affective Picture Paradigm*. Cognition and Emotion, 38(5), 801–817. https://doi.org/10.1080/02699931.2024.2319273
Raffagnato, A., Angelico, C., Valentini, P., Miscioscia, M., & Gatta, M. (2020). Using the Body When There Are No Words for Feelings: Alexithymia and Somatization in Self-Harming Adolescents. Frontiers in Psychiatry, 11, Article 262. https://doi.org/10.3389/fpsyt.2020.00262
Reininger, K. M., Biel, H. M., Hennig, T., Zitzmann, S., Weigel, A., Spitzer, C., Toussaint, A., & Löwe, B. (2023). Beliefs about emotions predict psychological stress related to somatic symptoms. The British Journal of Clinical Psychology, 62(4), 699–716. https://doi.org/10.1111/bjc.12438
Schwarzer, N.-H., Nolte, T., Fonagy, P., & Gingelmaier, S. (2021). Mentalizing mediates the association between emotional abuse in childhood and potential for aggression in non-clinical adults. Child Abuse & Neglect, 115, Article 105018. https://doi.org/10.1016/j.chiabu.2021.105018
Schwarzer, N.-H., Nolte, T., Fonagy, P., & Gingelmaier, S. (2022). Self-Rated Mentalizing Mediates the Relationship Between Stress and Coping in a Non-Clinical Sample. Psychological Reports, 125(2), 742–762. https://doi.org/10.1177/0033294121994846
Sonnby-Borgström, M. (2009). Alexithymia as Related to Facial Imitation, Mentalization, Empathy, and Internal Working Models-of-Self and -Others. Neuropsychoanalysis, 11(1), 111–128. https://doi.org/10.1080/15294145.2009.10773602
Spink, G. L., Jorgensen, R. S., & Cristiano, S. (2018). Cognitive and affective factors predicting daily somatic complaints in college students. Journal of Counseling Psychology, 65(1), 110–119. https://doi.org/10.1037/cou0000229
Teixeira, R. J., Brandão, T., & Dores, A. R. (2022). Academic stress, coping, emotion regulation, affect and psychosomatic symptoms in higher education. Current Psychology, 41(11), 7618–7627. https://doi.org/10.1007/s12144-020-01304-z
Valickas, G., Želvienė, P., & Grakauskas, Ž. (2010). Psychometric characteristics of the improved four-factor coping with stress questionnaire. Psichologija, 41, 96–110. https://doi.org/10.15388/Psichol.2010.0.2576
World Health Organization. (2016). International statistical classification of diseases and related health problems (10th ed.). https://icd.who.int/browse10/2016/en